Varicocele
A varicocele is an abnormal dilation of the pampiniform venous plexus within the spermatic cord, found in approximately 15% of all men, with prevalence increasing to 35% in men with primary inferti…
A varicocele is an abnormal dilation of the pampiniform venous plexus within the spermatic cord, found in approximately 15% of all men, with prevalence increasing to 35% in men with primary infertility and up to 80% in men with secondary infertility.[1-2] Most varicoceles are left-sided (85–90%) due to the anatomy of the left testicular venous drainage into the left renal vein.[1][3] The following is a clinically organized summary for emergency medicine and primary care evaluation.
1. History
- Onset, duration, and character of scrotal symptoms (most are asymptomatic and found incidentally)[1]
- Dull ache or scrotal heaviness, often worse with prolonged standing or exertion, improved with recumbency[1][4]
- Fertility history: duration of attempting conception, prior pregnancies, partner's fertility status[5]
- Sexual history and prior STI screening (to differentiate from epididymitis)
- History of trauma to the scrotum
- Timing relative to puberty in adolescents (varicoceles become more common as puberty begins)[6]
- Ask about rapid onset of new right-sided or bilateral scrotal swelling (may suggest secondary cause)[1]
2. Alarm Features
- Isolated right-sided varicocele → must evaluate for retroperitoneal mass (e.g., renal cell carcinoma) compressing the IVC or right gonadal vein[1]
- New-onset varicocele in an older man (>40 years) → consider retroperitoneal or pelvic malignancy causing venous obstruction
- Varicocele that does not decompress in the supine position → suggests venous obstruction from a mass[5]
- Acute severe scrotal pain → rule out testicular torsion (surgical emergency, salvage rate ~90% within 6 hours)[1]
- Hard, non-tender testicular mass → concern for testicular cancer[1]
- Constitutional symptoms (weight loss, fever, night sweats) → malignancy workup
3. Medications
- No specific medications cause varicoceles
- Symptomatic management of pain: NSAIDs (ibuprofen 400–600 mg PO q6–8h) and scrotal support
- Acetaminophen as an alternative analgesic
- No role for empiric antibiotics unless epididymitis is suspected
- In the fertility context, antioxidant supplements (e.g., vitamin C, vitamin E, CoQ10) have been studied but lack definitive evidence for routine use
4. Diet
- No specific dietary triggers or restrictions for varicocele
- General recommendations for men with fertility concerns: balanced diet rich in antioxidants, adequate hydration
- Avoidance of excessive heat exposure to the scrotum (hot tubs, saunas, laptops on lap) may be relevant in the fertility context given the role of scrotal hyperthermia in varicocele pathophysiology[2]
5. Review of Systems
- GU: dysuria, hematuria, urethral discharge, testicular pain, erectile dysfunction
- Constitutional: fever, weight loss, fatigue (malignancy red flags)
- GI/Abdominal: flank pain, abdominal mass (retroperitoneal pathology)
- Musculoskeletal: groin or inguinal pain (hernia vs. referred pain)
- Reproductive: libido changes, prior semen analyses, hypogonadal symptoms (fatigue, decreased energy — larger varicoceles may impact testosterone production)[2][5]
6. Collateral History and Family History
- Family history of infertility or varicocele
- Family history of renal cell carcinoma or retroperitoneal malignancy (relevant if isolated right-sided or new-onset varicocele)
- Partner's reproductive history and gynecologic evaluation status
- Social context: occupations requiring prolonged standing may exacerbate symptoms
7. Risk Factors
- Age: typically presents during puberty (peak onset 15–25 years)[6-7]
- Tall stature (longer gonadal vein)
- Left-sided predominance due to the left gonadal vein draining into the left renal vein at a right angle[1][3]
- Incompetent or absent venous valves in the internal spermatic vein
- Possible genetic predisposition[8]
- No clear modifiable lifestyle risk factors
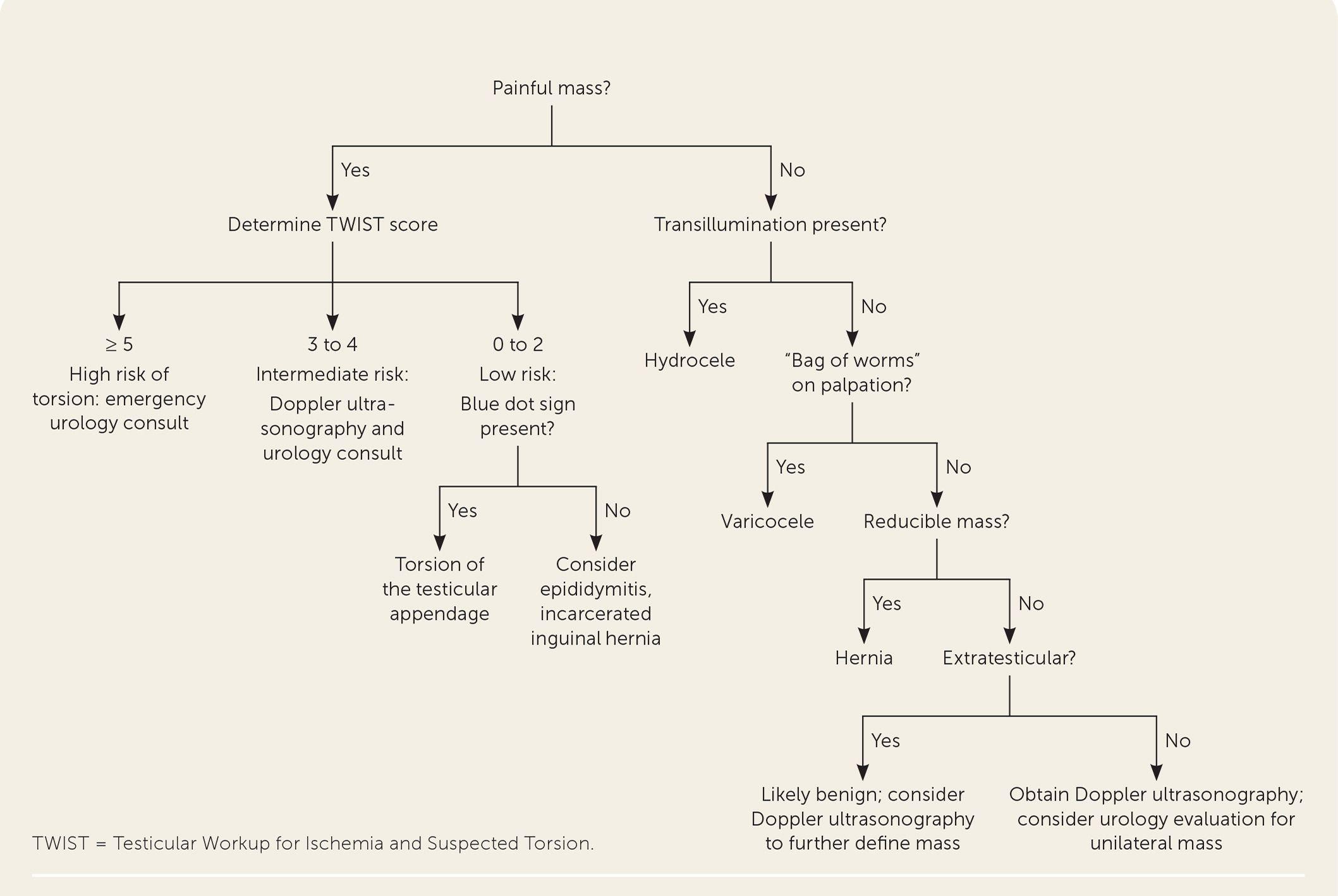
8. Differential Diagnosis
- The following algorithm from the AAFP provides a systematic approach to evaluating scrotal masses:
- Hydrocele: painless, smooth, fluctuant, transilluminates; extratesticular[1]
- Spermatocele/epididymal cyst: painless cystic mass at the head of the epididymis; transilluminates
- Inguinal hernia: reducible mass, palpable impulse with Valsalva, extends into inguinal canal[4]
- Epididymitis: painful, gradual onset, tenderness over epididymis, positive Prehn sign, often infectious[1]
- Testicular torsion: acute severe pain, high-riding testis, absent cremasteric reflex — surgical emergency[1]
- Testicular cancer: firm, non-tender, unilateral intratesticular mass; does not transilluminate[1]
- Torsion of testicular appendage: gradual onset of superior pole pain, "blue dot" sign[1]
9. Past Medical History
- Prior scrotal surgery or varicocele repair (recurrence rate varies by technique)
- History of cryptorchidism (associated with both infertility and testicular cancer risk)
- Prior fertility evaluations or semen analyses
- Chronic conditions: renal disease, retroperitoneal surgery, or known malignancy
- History of DVT or venous insufficiency
10. Physical Exam
- Examine patient standing in a warm room; inspect and palpate both hemiscrotums[3][5]
- Classic finding: "bag of worms" palpable above and posterior to the testis[1][5]
- Perform Valsalva maneuver — varicocele should increase in size with Valsalva and decompress when supine[3][5]
Grading (WHO)
- Grade I: palpable only with Valsalva
- Grade II: palpable at rest in upright position
- Grade III: visible at rest in upright position
- Assess testicular size bilaterally — ipsilateral testicular atrophy suggests varicocele-related damage[5]
- Check cremasteric reflex (to rule out torsion)[1]
- Palpate inguinal canals for hernia
- Transilluminate to differentiate from hydrocele[1]
- Abdominal exam if concern for retroperitoneal mass
11. Lab Studies
- Routine labs are generally not needed for uncomplicated varicocele[1]
If fertility concern
- Semen analysis (at least two) — assess count, motility, morphology[5]
- FSH, LH, testosterone — to evaluate for hypogonadism; elevated FSH may indicate impaired spermatogenesis[5]
- Inhibin B — marker of Sertoli cell function (research setting)
- If testicular mass suspected: AFP, β-hCG, LDH (tumor markers)[1]
- If epididymitis suspected: urinalysis, urine culture, GC/chlamydia NAAT
- Sperm DNA fragmentation testing is emerging but not yet routine[8]
12. Imaging
- Scrotal ultrasound with color Doppler is the first-line imaging modality when physical exam is inconclusive[5][9-10]
- Diagnostic criteria: spermatic veins >2.5–3.0 mm in diameter with retrograde flow on Valsalva[5]
- Also assesses testicular volume discrepancy
- Imaging is not indicated for routine screening if the varicocele is clearly palpable[5][11]
- CT abdomen/pelvis: indicated for isolated right-sided varicocele or new-onset varicocele in older men to rule out retroperitoneal mass[1]
- Spermatic venography: reserved for recurrent or persistent varicocele post-repair[5]
- Shear wave elastography is an emerging modality under investigation[8]
13. Special Tests
- TWIST score (Testicular Workup for Ischemia and Suspected Torsion): useful when acute scrotal pain is the presenting complaint to risk-stratify for torsion[1]
- Orchidometer or ultrasound volumetry for serial testicular volume measurement in adolescents[12]
- Peak retrograde flow (PRF) on Doppler: PRF >38 cm/s may indicate higher risk of testicular dysfunction in adolescents[6]
14. ECG
- Not applicable for varicocele evaluation
15. Assessment
- Varicocele is a common, usually benign condition that is most often asymptomatic and discovered incidentally or during infertility evaluation.[1] Key clinical considerations:
- Only clinically palpable varicoceles have been clearly associated with infertility[5][11]
- Subclinical varicoceles (detected only by imaging) have no demonstrated benefit from treatment[5][11]
- The mechanism of fertility impairment is multifactorial: scrotal hyperthermia, oxidative stress, testicular hypoxia, and blood-testis barrier disruption[2]
- Larger varicoceles may have a greater impact on semen parameters and testosterone production[2][5]
- Severity stratification should incorporate varicocele grade, testicular volume asymmetry, semen parameters, and hormonal profile
16. Treatment Plan
Conservative management (majority of patients)
- Scrotal support (supportive underwear)
- NSAIDs for symptomatic pain
- Observation with serial semen analyses every 1–2 years for young men with normal semen parameters[5]
- Indications for varicocele repair (per AUA/ASRM guidelines):[5][11]
- Palpable varicocele + known infertility + abnormal semen parameters + female partner with normal or treatable fertility
- Palpable varicocele + pain refractory to conservative measures
- Adolescents with ipsilateral testicular volume loss (≥20% asymmetry) or abnormal semen analysis[5-6]
Surgical options
- Microsurgical subinguinal varicocelectomy — gold standard; lowest recurrence (~1%) and complication rates[5][8]
- Inguinal microsurgical approach — similar outcomes
- Laparoscopic varicocelectomy — higher recurrence than microsurgical
- Percutaneous embolization — minimally invasive alternative; comparable efficacy[5]
Repair is NOT indicated for
- Subclinical (non-palpable) varicoceles
- Normal semen quality
- Isolated teratozoospermia
- Time to improvement in semen parameters post-repair: approximately 3–6 months.[5]
17. Disposition
- Outpatient management is appropriate for the vast majority of varicoceles[13]
Urology referral indications
- Infertility with palpable varicocele and abnormal semen parameters[5][11]
- Symptomatic varicocele refractory to conservative measures
- Adolescent with testicular volume asymmetry or abnormal semen analysis[5][12]
- Isolated right-sided varicocele (after retroperitoneal imaging)[1]
- Suspicion of testicular mass or malignancy[1]
- Emergency department disposition: varicocele itself is not an emergency; however, if acute scrotal pain is the presentation, torsion must be excluded before discharge[1]
18. Follow Up / Return Precautions
- Adolescents: annual follow-up with testicular volume measurement and/or semen analysis (Tanner V) until paternity is achieved[5][12]
- Adults with untreated varicocele and fertility concerns: semen analysis every 1–2 years[5]
- Post-repair: repeat semen analysis at 3–6 months; if no improvement by 6 months, further evaluation warranted[5]
Return precautions (counsel patients to return for)
- Acute onset of severe scrotal pain (torsion concern)
- New hard testicular mass
- Worsening scrotal swelling or pain despite conservative measures
- Constitutional symptoms (weight loss, fever)
- Expected course: most varicoceles are stable and benign; surgical repair, when indicated, has a low complication rate and is associated with improvement in semen parameters in the majority of patients[5]
References
1. Scrotal Masses. — Langan RC, Puente MEE. American Family Physician. 2022.
2. Effect of Varicoceles on Spermatogenesis. — Kang C, Punjani N, Lee RK, Li PS, Goldstein M. Seminars in Cell & Developmental Biology. 2022.
3. Surgical or Radiological Treatment for Varicoceles in Subfertile Men. — Persad E, O'Loughlin CA, Kaur S, et al. The Cochrane Database of Systematic Reviews. 2021.
4. Inguinal Hernias: Diagnosis and Management. — Shakil A, Aparicio K, Barta E, Munez K. American Family Physician. 2020.
5. Report on Varicocele and Infertility: A Committee Opinion. — Fertility and Sterility. 2014.
6. Management and Treatment of Varicocele in Children and Adolescents: An Endocrinologic Perspective. — Cannarella R, Calogero AE, Condorelli RA, et al. Journal of Clinical Medicine. 2019.
7. Adolescent Varicocele: A Surgical Conundrum. — Beland LE, Davis MF, Aiyar S, et al. Fertility and Sterility. 2026.
8. Recent Trends in the Management of Varicocele. — Takács T, Szabó A, Kopa Z. Journal of Clinical Medicine. 2025.
9. Imaging of the Acute Scrotum: Keys to a Rapid Diagnosis of Acute Scrotal Disorders. — Sweet DE, Feldman MK, Remer EM. Abdominal Radiology. 2020.
10. ACR Appropriateness Criteria® Newly Diagnosed Palpable Scrotal Abnormality. — Khatri G, Bhosale PR, Robbins JB, et al. Journal of the American College of Radiology : JACR. 2022.
11. Diagnosis and Treatment of Infertility in Men: AUA/ASRM Guideline Part II. — Schlegel PN, Sigman M, Collura B, et al. Fertility and Sterility. 2021.
12. Evaluation and Management of the Adolescent Varicocele. — Kolon TF. The Journal of Urology. 2015.
13. Evaluation of Scrotal Masses. — Crawford P, Crop JA. American Family Physician. 2014.