Ventricular Escape Rhythm
A ventricular escape rhythm (idioventricular rhythm) is a life-sustaining backup rhythm originating from the ventricular myocardium or distal His-Purkinje system, typically firing at an intrinsic r…
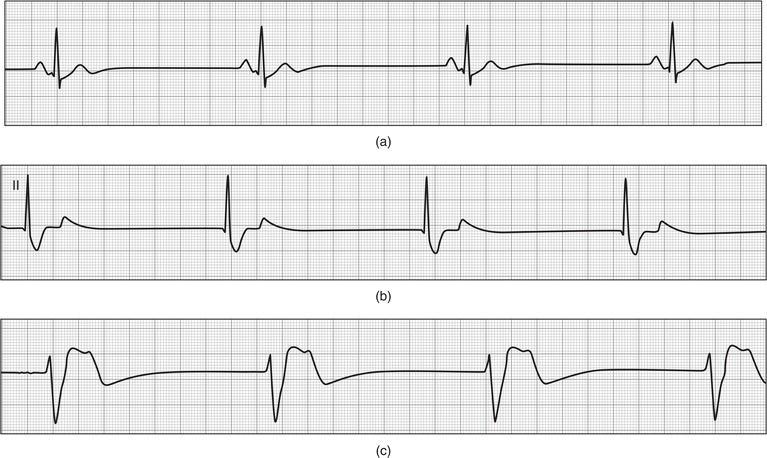
A ventricular escape rhythm (idioventricular rhythm) is a life-sustaining backup rhythm originating from the ventricular myocardium or distal His-Purkinje system, typically firing at an intrinsic rate of 20–40 bpm when all higher pacemaker sites (sinus node, AV node/junction) fail or when complete AV block prevents supraventricular impulses from reaching the ventricles.[1-2] It represents the lowest level of the cardiac pacemaker hierarchy and is a marker of serious conduction system disease.
The following figure illustrates the hierarchy of escape rhythms, with panel (c) demonstrating the characteristic wide-complex, slow ventricular escape rhythm:
1. History
- Onset and duration of symptoms: acute vs. chronic; sudden vs. gradual
- Syncope or presyncope — most critical symptom; ask about frequency, duration, prodrome, and positional triggers
- Lightheadedness, dizziness, fatigue, exercise intolerance, dyspnea on exertion
- Chest pain (ischemic etiology), palpitations
- Recent medication changes — new AV nodal blockers, dose increases, or polypharmacy
- Tick exposure or erythema migrans rash (Lyme carditis)[4]
- Recent cardiac surgery, catheterization, or TAVR[5]
- History of myocardial infarction (especially inferior MI)
- Symptoms of heart failure: orthopnea, PND, lower extremity edema
2. Alarm Features
- Syncope or near-syncope — suggests hemodynamic compromise from inadequate cardiac output
- Heart rate <30 bpm or prolonged asystolic pauses (≥3 seconds)[6-7]
- Hypotension, altered mental status, signs of cardiogenic shock
- Chest pain suggesting acute coronary syndrome
- Wide QRS escape rhythm (infranodal block) — more unpredictable and less responsive to atropine than junctional escapes[2][4]
- New-onset heart failure symptoms
- Absence of a reliable escape rhythm upon pacemaker inhibition — 24% of patients with complete AV block had no reliable escape, developing symptoms after a mean of ~7 seconds[8]
3. Medications
Causative/Contributing Agents
- Beta-blockers (including ophthalmic formulations)
- Non-dihydropyridine calcium channel blockers (verapamil, diltiazem)
- Digoxin — toxicity causes AV block; treat with digoxin-specific Fab antibodies
- Antiarrhythmics: amiodarone, sotalol, flecainide, propafenone
- Fingolimod (sphingosine 1-phosphate receptor modulator)
- Clonidine, ivabradine, acetylcholinesterase inhibitors (donepezil)
Acute Treatment Agents
- Atropine 0.5 mg IV q3–5 min (max 3 mg) — often ineffective for infranodal block
- Epinephrine or dopamine infusion for refractory bradycardia
- Isoproterenol — may improve infranodal escape rates via catecholamine effect
- Do NOT give atropine to heart transplant patients (risk of paradoxical block/sinus arrest)[9]
Contraindicated Medications
- Avoid AV nodal blockers in the absence of a functioning pacemaker[9]
- Calcium channel blockers (verapamil, diltiazem) are potentially harmful in wide-complex rhythms of unknown origin[11]
4. Diet
- No specific dietary triggers for ventricular escape rhythm
- Ensure adequate potassium and magnesium intake — electrolyte abnormalities (hyperkalemia in particular) can worsen conduction disease[10]
- Patients on digoxin should avoid excessive potassium depletion (increases digoxin toxicity risk)
- Adequate hydration to maintain preload in the setting of low cardiac output
5. Review of Systems
- Cardiovascular: syncope, presyncope, palpitations, chest pain, dyspnea, exercise intolerance, edema
- Neurologic: dizziness, confusion, seizure-like activity (Stokes-Adams attacks)
- Musculoskeletal: muscle weakness (neuromuscular diseases — myotonic dystrophy, Kearns-Sayre syndrome)[5][7]
- Dermatologic: erythema migrans (Lyme disease)[4]
- Constitutional: fatigue, weight changes (hypothyroidism)
- Respiratory: dyspnea (heart failure, sarcoidosis)
6. Collateral History and Family History
- Family history of sudden cardiac death, conduction disease, or pacemaker implantation
- Hereditary conditions: congenital complete heart block (associated with maternal anti-Ro/SSA antibodies in neonatal lupus), neuromuscular dystrophies[7][12]
- Lamin A/C gene mutations (Emery-Dreifuss, limb-girdle muscular dystrophy) — associated with progressive conduction disease[4]
- Collateral from witnesses regarding syncopal episodes (duration, seizure-like activity, recovery time)
- Medication list from pharmacy or family members
7. Risk Factors
- Advanced age — degenerative fibrosis of the conduction system is the most common cause[4]
- Chronic hypertension and diabetes mellitus[4]
- Coronary artery disease — especially prior inferior MI (AV nodal block) or anterior MI (infranodal block)[4]
- Prior cardiac surgery or TAVR[5]
- Infiltrative diseases: cardiac sarcoidosis, amyloidosis[4]
- Neuromuscular diseases: myotonic dystrophy, Kearns-Sayre syndrome[7]
- Infectious: Lyme disease in endemic areas[4]
- Polypharmacy with multiple AV nodal blocking agents[13]
- Autoimmune: SLE, rheumatoid arthritis[5]
8. Differential Diagnosis
- Complete (third-degree) AV block with ventricular escape — most common context
- Junctional escape rhythm — narrow QRS, rate 40–60 bpm (higher in the pacemaker hierarchy)[2]
- Accelerated idioventricular rhythm (AIVR) — rate 40–100 bpm, often benign and seen in reperfusion after MI; distinguished from escape rhythm by faster rate[14-15]
- Slow ventricular tachycardia — can mimic escape rhythm; clinical context and rate help differentiate
- Hyperkalemia — can produce wide-complex bradycardia mimicking ventricular escape
- Pacemaker malfunction — failure to capture or sense in a pacemaker-dependent patient
- Severe sinus node dysfunction with failure of junctional escape
- Drug toxicity (digoxin, beta-blocker, calcium channel blocker overdose)[9]
9. Past Medical History
- Prior MI, heart failure, cardiomyopathy
- Previous episodes of syncope or documented bradycardia
- Prior cardiac surgery (valve replacement, CABG)
- Known conduction disease (bundle branch block, bifascicular block)
- Existing pacemaker or ICD
- Neuromuscular disease
- Autoimmune or infiltrative disease
- Thyroid disease (hypothyroidism)
10. Physical Exam
Vital Signs
- Bradycardia (typically 20–40 bpm)
- Hypotension if hemodynamically significant
Key Findings
- Cannon A waves in the JVP — intermittent, due to atrial contraction against a closed tricuspid valve (AV dissociation)
- Varying intensity of S1 — hallmark of AV dissociation
- Varying pulse volume — beat-to-beat variation in stroke volume
- Signs of heart failure: elevated JVP, pulmonary crackles, peripheral edema
- Altered mental status if cerebral hypoperfusion is present
- Skin exam: erythema migrans (Lyme), signs of neuromuscular disease
11. Lab Studies
- Basic metabolic panel — potassium (hyperkalemia), calcium, magnesium
- Troponin — rule out acute MI as cause of AV block[16]
- Digoxin level — if on digoxin therapy[5]
- TSH — hypothyroidism can contribute to conduction disease[4]
- Lyme serologies (ELISA + Western blot) — in endemic areas or with suggestive history[4]
- BNP/NT-proBNP — if heart failure suspected
- ACE level, inflammatory markers — if sarcoidosis suspected
- CBC — infection workup
12. Imaging
- Transthoracic echocardiography — first-line; assess LV function, wall motion abnormalities, valvular disease, infiltrative disease[16]
- Cardiac MRI — gold standard for detecting myocardial scar, sarcoidosis, or infiltrative cardiomyopathy
- Coronary angiography — if acute coronary syndrome is suspected as the cause of AV block[16]
- Chest X-ray — cardiomegaly, pulmonary congestion, hilar lymphadenopathy (sarcoidosis)
- Imaging is unnecessary if the etiology is clearly drug-related and reversible
13. Special Tests
- Electrophysiology study (EPS) — can localize the level of block (AV nodal vs. intra-Hisian vs. infra-Hisian); HV interval ≥70 ms suggests infranodal disease warranting pacing[12]
- Ambulatory ECG monitoring (Holter or event monitor) — for intermittent symptoms
- Exercise stress testing — AV block that worsens with exercise suggests infranodal disease
- Carotid sinus massage — if carotid sinus hypersensitivity is suspected
- Tilt-table testing — for neurally mediated syncope evaluation
14. ECG
Characteristic ECG Features
- Wide QRS complexes (≥120 ms), often bizarre morphology — reflecting ventricular origin of depolarization[2-3]
- Regular R-R intervals at a rate of 20–40 bpm[1][15]
- AV dissociation — P waves and QRS complexes march independently; P-wave rate exceeds QRS rate[16]
- No fixed relationship between P waves and QRS complexes
- Varying PR intervals (when P waves are visible)
Dangerous Patterns to Recognize
- Prolonged asystolic pauses (≥3 seconds)[6]
- Very slow escape rate (<20 bpm) — high risk for cardiac arrest
- Alternating bundle branch block morphology — suggests severe infranodal disease with high risk of sudden complete block[5]
- QT prolongation in the setting of bradycardia — risk for torsades de pointes
- Distinguishing from AIVR: AIVR has a rate of 40–100 bpm and is often associated with fusion beats and a "warm-up" phenomenon; ventricular escape rhythm is slower and represents a passive, failsafe mechanism[1][14]
15. Assessment
- A ventricular escape rhythm is not a primary diagnosis but a manifestation of failure of all higher pacemaker sites, most commonly due to complete AV block. It is a life-sustaining but unreliable rhythm. Key clinical considerations:
- Infranodal block (wide QRS escape) carries worse prognosis than AV nodal block (narrow QRS junctional escape) — more unpredictable, slower rate, less responsive to atropine[2][4]
- Patients without a reliable escape rhythm (24% in one study) are at highest risk for sudden death[8]
- Even patients with a reliable escape should be considered pacemaker-dependent, as escape reliability can vary over time[8]
- Complications include syncope (Stokes-Adams attacks), heart failure from chronotropic incompetence, and sudden cardiac death
16. Treatment Plan
Initial Stabilization
- ABCs, continuous cardiac monitoring, IV access
- Atropine 0.5 mg IV q3–5 min (max 3 mg) — first-line per AHA guidelines; note: often ineffective for infranodal block[10]
- If atropine fails: transcutaneous pacing as a bridge (may require sedation in conscious patients)[10]
- Epinephrine infusion (2–10 mcg/min) or dopamine infusion (5–20 mcg/kg/min) if pacing is unavailable or as a bridge[10]
- Identify and treat reversible causes: stop offending medications, correct hyperkalemia, treat ischemia, administer digoxin-specific Fab for digoxin toxicity[4][9]
Definitive Treatment
- Temporary transvenous pacing for hemodynamically unstable patients as a bridge to permanent pacing[10]
- Permanent pacemaker implantation — Class I indication for acquired third-degree AV block not attributable to reversible causes, regardless of symptoms[4-5]
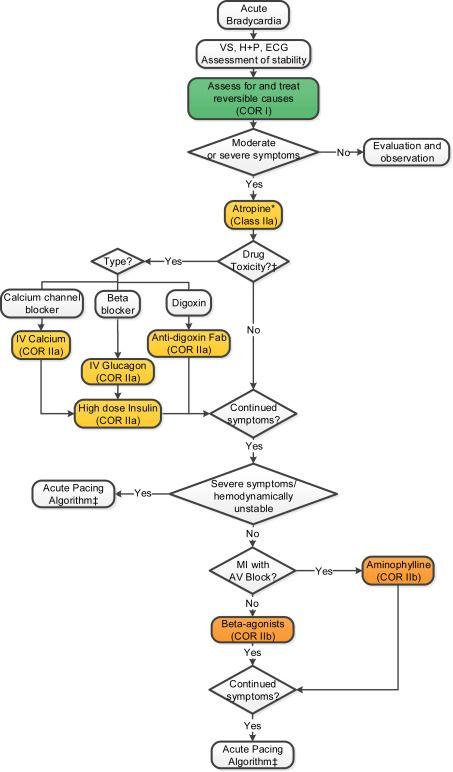
- The 2018 ACC/AHA/HRS Bradycardia Guidelines provide the following algorithm for acute management:
- View full figure Figure 4. Acute Bradycardia Algorithm 2018 ACC/AHA/HRS Guideline on The Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. J Am Coll Cardiol. August 19, 2019.
Pacemaker Indications (Class I)
- Third-degree or advanced second-degree AV block with symptomatic bradycardia
- Asymptomatic third-degree AV block with escape rate <40 bpm or infranodal escape
- Asystolic pauses ≥3 seconds in awake patients
- AV block requiring medically necessary drugs that cause symptomatic bradycardia
17. Disposition
Admission Criteria
- All patients with new-onset ventricular escape rhythm require admission with continuous telemetry
- Hemodynamic instability → ICU/CCU with temporary pacing capability
- Symptomatic bradycardia (syncope, presyncope, heart failure)
- Pending permanent pacemaker implantation
Observation Indications
- Drug-related AV block with expected reversibility after drug washout — though ~50% recur and ultimately need permanent pacing[9][13]
- Lyme carditis — median resolution 6 days (range up to 42 days); temporary pacing needed in ~40%[4]
Discharge Criteria
- Stable permanent pacemaker in place with appropriate function
- Reversible cause fully treated with documented resolution of AV block
Specialist Consultation
- Cardiology/Electrophysiology — all patients with ventricular escape rhythm
- Infectious disease — if Lyme carditis suspected
- Toxicology — for drug overdose
18. Follow Up / Return Precautions
Follow-Up Timing
- Post-pacemaker implantation: wound check at 1–2 weeks, device interrogation at 1 month, then every 6–12 months
- If discharged after reversible cause: close cardiology follow-up within 1–2 weeks with repeat ECG
- Return Precautions — instruct patients to return immediately for:
- Syncope or near-syncope
- Recurrent dizziness, lightheadedness, or confusion
- New chest pain or shortness of breath
- Palpitations or sensation of very slow heartbeat
Patient Counseling
- Ventricular escape rhythm is a sign of serious conduction system disease that typically requires a permanent pacemaker
- Avoid driving until cleared by cardiology (syncope risk)
- Medication reconciliation — ensure no unnecessary AV nodal blockers are continued without pacemaker protection
References
1. ECG Clues for Diagnosing Ventricular Tachycardia Mechanism. — Riley MP, Marchlinski FE. Journal of Cardiovascular Electrophysiology. 2008.
2. The Evaluation and Management of Bradycardia. — Mangrum JM, DiMarco JP. The New England Journal of Medicine. 2000.
3. Electrocardiographic Differential Diagnosis of Bradyarrhythmia. — Megan Starling, William J. Brady The Electrocardiagram in Emergency and Acute Care. 2023.
4. 2018 ACC/AHA/HRS Guideline on The evaluation and Management Of patients With Bradycardia and Cardiac conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Writing Committee Members, Kusumoto FM, Schoenfeld MH, et al. Heart Rhythm. 2019.
5. 2018 ACC/AHA/HRS Guideline on The Evaluation and Management Of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Kusumoto FM, Schoenfeld MH, Barrett C, et al. Journal of the American College of Cardiology. 2019.
6. 2012 ACCF/AHA/HRS Focused Update Incorporated Into the ACCF/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. — Epstein AE, DiMarco JP, Ellenbogen KA, et al. Journal of the American College of Cardiology. 2013.
7. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons. — Epstein AE, DiMarco JP, Ellenbogen KA, et al. Journal of the American College of Cardiology. 2008.
8. Comparison Between Patients With and Without Reliable Ventricular Escape Rhythm in the Presence of Long Standing Complete Atrioventricular Block. — Rosenheck S, Bondy C, Weiss AT, Gotsman MS. Pacing and Clinical Electrophysiology : PACE. 1993.
9. Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association. — Tisdale JE, Chung MK, Campbell KB, et al. Circulation. 2020.
10. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Wigginton JG, Agarwal S, Bartos JA, et al. Circulation. 2025.
11. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Heart Rhythm. 2018.
12. Pacemakers. — Aldaas OM, Roberge-Lacharite AS, Birgersdotter-Green U. NEJM Evidence. 2025.
13. Clinical Significance and Management of Atrioventricular Block Associated With Bradycardic/Antiarrhythmic Drug Therapy: Drug‐Induced or Drug‐Revealed?. — Sfairopoulos D, Bazoukis G, Sideris S, et al. Journal of Cardiovascular Electrophysiology. 2025.
14. 2019 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on Catheter Ablation of Ventricular Arrhythmias: Executive Summary. — Cronin EM, Bogun FM, Maury P, et al. Heart Rhythm. 2020.
15. ACC/AHA/HRS 2006 Key Data Elements and Definitions for Electrophysiological Studies and Procedures: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (ACC/AHA/HRS Writing Committee to Develop Data Standards on Electrophysiology). — Buxton AE, Calkins H, Callans DJ, et al. Journal of the American College of Cardiology. 2006.
16. An Unusual Cause of Atrioventricular Block. — Rajendran K, Alphonse AJ, Desabandhu V. JAMA Internal Medicine. 2025.
17. 2018 ACC/AHA/HRS Guideline on The Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. — Kusumoto FM, Schoenfeld MH, Barrett C, et al. Journal of the American College of Cardiology. 2019.