Ventricular Tachycardia (Stable)
Stable Ventricular Tachycardia (VT)
Stable Ventricular Tachycardia (VT)
Stable VT is defined as sustained monomorphic VT (≥3 consecutive ventricular complexes at ≥100 bpm with QRS ≥120 ms) that is hemodynamically tolerated — meaning the patient maintains adequate blood pressure, mentation, and perfusion.[1-2] Despite hemodynamic stability, VT remains an inherently unstable rhythm with risk of deterioration into VF.[3]
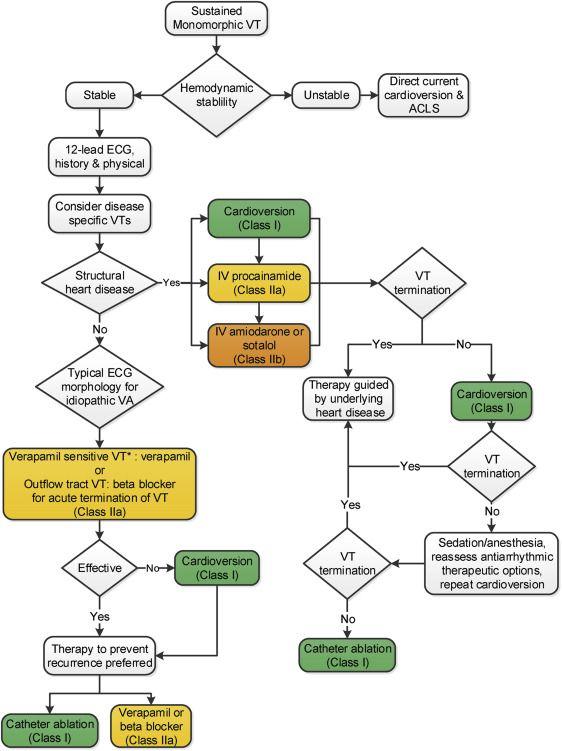
The following figure from the 2017 AHA/ACC/HRS guidelines illustrates the management algorithm for sustained monomorphic VT, stratified by hemodynamic stability and presence of structural heart disease:
View full figure Figure 2. Management of Sustained Monomorphic VT 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. October 1, 2018.
1. History
- Onset and duration: Sudden vs. gradual onset, duration of symptoms, prior episodes
- Symptom characterization: Palpitations, chest pain/pressure, dyspnea, lightheadedness, presyncope, near-syncope
- Triggers: Exertion, emotional stress, caffeine, stimulant use, recent medication changes
- Associated symptoms: Diaphoresis, nausea, jaw/arm pain (ischemia), recent illness with vomiting/diarrhea (electrolyte depletion)
- Important negatives: Syncope (suggests hemodynamic instability), seizure-like activity, witnessed cardiac arrest
- Cardiac history: Prior MI, heart failure, cardiomyopathy, prior arrhythmias, ICD/pacemaker, prior ablation[4-5]
- Medication reconciliation: Recent changes in antiarrhythmics, diuretic dose adjustments, new QT-prolonging drugs[3][6]
2. Alarm Features
- Hypotension (SBP <80 mmHg), altered mental status, or signs of poor perfusion → immediate synchronized cardioversion[2][7]
- Chest pain with ST changes suggesting acute coronary syndrome
- Polymorphic VT or VT degenerating into VF
- VT storm (≥3 episodes in 24 hours)[8]
- Signs of cardiogenic shock: cool extremities, mottled skin, pulmonary edema
- Syncope or near-syncope during the episode
- Very rapid rates (>200 bpm) with impending hemodynamic collapse
3. Medications
Medications that can cause/exacerbate VT
- Class IC antiarrhythmics (flecainide, propafenone) — especially with structural heart disease
- Digoxin toxicity (triggered activity)
- QT-prolonging drugs (antipsychotics, certain antibiotics, antiemetics)
- Sympathomimetics (cocaine, methamphetamine, ephedrine)
- Theophylline toxicity
- Tricyclic antidepressants (sodium channel blockade)
- Acute treatment options (per AHA/ACC/HRS 2017 and AHA 2025 guidelines):[1-2][7][9]
- IV procainamide: 10 mg/kg at 50–100 mg/min (Class IIa) — most efficacious for stable monomorphic VT; monitor BP and QRS/QT
- IV amiodarone: 150 mg over 10 min, then infusion (Class IIb) — slower onset, risk of hypotension
- IV sotalol: Newer option without significant hypotension concerns (Class IIb)
- Synchronized cardioversion: Most effective at any point; requires procedural sedation[8-9]
Contraindicated medications
- Verapamil/diltiazem — potentially harmful in wide-complex tachycardia of unknown origin; can cause profound hypotension and cardiovascular collapse in VT
- Lidocaine — less effective than procainamide, amiodarone, or sotalol for hemodynamically tolerated VT; may be considered only in acute MI-related VT[7-8]
- Avoid co-administration of multiple antiarrhythmics (arrhythmogenic risk)[7]
4. Diet
- Not a primary factor in acute management
- Long-term: Adequate potassium and magnesium intake through diet (bananas, leafy greens, nuts) in patients on diuretics
- Avoid excessive caffeine and alcohol, which may lower arrhythmia threshold
- Patients on amiodarone should be counseled about iodine-rich foods (thyroid effects)
5. Review of Systems
- Cardiovascular: Palpitations, chest pain, dyspnea on exertion, orthopnea, PND, lower extremity edema
- Neurologic: Syncope, presyncope, dizziness, seizure-like activity
- GI: Recent vomiting, diarrhea (electrolyte depletion — strongly associated with hypokalemia-triggered VT)[6]
- Endocrine: Symptoms of thyroid disease (hyper/hypothyroidism)
- Psychiatric/Substance: Stimulant use, cocaine, energy drinks
- Constitutional: Fever (myocarditis), weight loss (malignancy, pheochromocytoma)
6. Collateral History and Family History
- Family history of sudden cardiac death (especially <50 years) — raises concern for inherited channelopathies (long QT, Brugada, CPVT) or cardiomyopathies (HCM, ARVC, DCM)[10]
- Family history of unexplained drowning, single-vehicle accidents, or SIDS
- Collateral from bystanders: Duration of episode, loss of consciousness, seizure activity
- ICD interrogation data if applicable
- Social history: Cocaine, methamphetamine, alcohol use
7. Risk Factors
- Structural heart disease — the most important risk factor; prior MI with scar is the most common substrate for sustained monomorphic VT[4-5][11]
- Reduced LVEF / heart failure[11]
- Nonischemic dilated cardiomyopathy
- Hypertrophic cardiomyopathy
- ARVC[10][12]
- Cardiac sarcoidosis
- Congenital heart disease (e.g., repaired tetralogy of Fallot)[4]
- Inherited channelopathies (long QT, Brugada, CPVT)[10]
- Electrolyte abnormalities: Hypokalemia (present in ~36% of VT/VF presentations), hypomagnesemia[6][8]
- Diuretic use (especially with recent dose increase — OR 21.9 for severe hypokalemia)[6]
- Drug toxicity (digoxin, class IC agents, cocaine)[3]
- Acute myocardial ischemia[4]
8. Differential Diagnosis
- A wide-complex tachycardia should be presumed to be VT if the diagnosis is unclear (Class I recommendation).[2][8]
- SVT with aberrant conduction (bundle branch block) — most common mimic; look for typical BBB morphology, prior ECGs for comparison[1][13]
- Pre-excited tachycardia (antidromic AVRT via accessory pathway) — history of WPW, delta waves on prior ECG
- Atrial fibrillation with pre-excitation — irregularly irregular wide-complex tachycardia; avoid AV nodal blockers
- Ventricular paced rhythm — check for pacemaker/ICD
- Hyperkalemia — can produce wide-complex rhythm mimicking VT; check potassium urgently[7]
- Sodium channel blocker toxicity (TCA overdose, flecainide) — wide QRS with rightward axis[3]
- ECG artifact — can mimic VT; inappropriate treatments have been administered when artifact was not recognized[4]
Distinguishing features favoring VT
- AV dissociation (cannon A waves, variable S1)
- QRS >140 ms
- Concordance in precordial leads
- Monophasic R in aVR
- No RS complex in any precordial lead, or RS interval >100 ms
- Fusion or capture beats
9. Past Medical History
- Prior MI or coronary artery disease (scar-related reentry)
- Heart failure with reduced EF
- Prior VT/VF episodes, ICD shocks
- Cardiomyopathy (ischemic, dilated, hypertrophic, ARVC)
- Cardiac surgery (e.g., valve replacement, congenital heart repair)
- Prior catheter ablation for VT
- Chronic kidney disease (electrolyte shifts)
- Thyroid disease
- Medication list with attention to antiarrhythmics, diuretics, QT-prolonging agents
10. Physical Exam
- Vitals: Heart rate, blood pressure (confirm hemodynamic stability), SpO2, respiratory rate
Cardiovascular
- Cannon A waves in JVP (AV dissociation — pathognomonic for VT)
- Variable intensity of S1 (AV dissociation)
- S3/S4 gallop (heart failure)
- Murmurs (valvular disease, HCM)
- Signs of poor perfusion: cool extremities, delayed capillary refill, mottled skin
- Pulmonary: Crackles (pulmonary edema)
- Neurologic: Mental status assessment (altered mentation = unstable)
- Extremities: Edema, signs of peripheral vascular disease
- Surgical scars: Sternotomy (prior cardiac surgery), ICD/pacemaker pocket
11. Lab Studies
- Recommended labs to identify reversible causes and assess end-organ function:[5][14]
- Basic metabolic panel: Potassium, magnesium, calcium (hypokalemia present in ~36% of VT presentations)[6]
- Troponin: Rule out acute MI as trigger
- BNP/NT-proBNP: Assess for heart failure
- CBC: Anemia (can exacerbate ischemia)
- Renal function: BUN/creatinine (drug dosing, electrolyte context)
- Thyroid function: TSH (hyper/hypothyroidism)
- Digoxin level: If on digoxin
- Toxicology screen: If substance use suspected
- ABG/VBG: If concern for acidosis
- Lactate: If concern for hypoperfusion
12. Imaging
- Echocardiography — first-line to assess for structural heart disease, LVEF, wall motion abnormalities, valvular disease[5][15]
- Coronary angiography — if acute ischemia suspected as trigger[5]
- Cardiac MRI — gold standard for ARVC, myocarditis, sarcoidosis, scar characterization; typically performed after stabilization[5][16]
- CT coronary angiography — alternative to invasive angiography in select patients[5]
- Chest X-ray — assess for cardiomegaly, pulmonary edema
- Imaging is generally not needed emergently if the patient has known structural heart disease and a prior established diagnosis of VT.
13. Special Tests
- Brugada criteria / Vereckei algorithm — systematic ECG-based algorithms to differentiate VT from SVT[1][13]
- Adenosine trial — can be diagnostic and therapeutic in stable, regular, monomorphic wide-complex tachycardia; terminates SVT but not VT, allowing rhythm diagnosis[7][17]
- Electrophysiology study (EPS) — for definitive diagnosis, VT induction, and mapping for ablation[4][16]
- Signal-averaged ECG — may be useful in suspected ARVC[18]
- Genetic testing — if inherited channelopathy or cardiomyopathy suspected[16]
- Provocative testing — ajmaline/flecainide challenge for Brugada syndrome; exercise testing for CPVT[16][18]
14. ECG
- A 12-lead ECG during tachycardia is the first diagnostic test and should be obtained before any attempt at termination (Class I recommendation).[1][13][18]
Key ECG findings supporting VT
- Wide QRS (>140 ms)
- AV dissociation (P waves marching through at independent rate)
- Fusion beats and capture beats
- Positive or negative concordance across precordial leads
- Monophasic R wave in aVR
- Absence of RS complex in all precordial leads
- RS interval >100 ms in any precordial lead
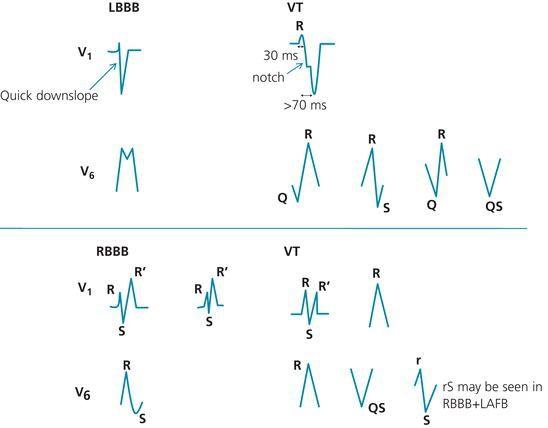
- LBBB morphology with notched S descent in V1, R >30 ms, or Q wave in V6
- RBBB morphology with monophasic R or qR in V1, QS in V6
Dangerous patterns to recognize
- Polymorphic VT / torsades de pointes (waxing/waning QRS amplitude with QT prolongation)
- Brugada pattern (coved ST elevation V1–V3)
- Epsilon waves (ARVC)
- Prolonged QT interval on baseline ECG
- The following figure illustrates morphologic differences between SVT with aberrancy and VT:
15. Assessment
- Severity stratification: Hemodynamically stable VT still carries significant risk — up to 40% recurrence within 2 years in patients with structural heart disease, with associated mortality risk[4]
- Typical presentation: Palpitations, mild dyspnea, chest discomfort in a patient with known structural heart disease and preserved consciousness
- Atypical presentations: Asymptomatic VT detected on telemetry; VT presenting as "SVT" in young patients without known heart disease (consider idiopathic VT)
- Complications: Hemodynamic deterioration, degeneration to VF, cardiogenic shock, end-organ damage, cardiac arrest
- Key distinction: Presence vs. absence of structural heart disease fundamentally alters prognosis and management[2][4]
16. Treatment Plan
Initial stabilization
- Continuous cardiac monitoring, IV access, defibrillator at bedside
- Obtain 12-lead ECG during tachycardia before any intervention
- Correct reversible causes: replete K⁺ to >4.0 mEq/L, Mg²⁺ to >2.0 mg/dL
Pharmacologic termination (if stable and time permits)
- Procainamide (preferred): 10 mg/kg IV at 50–100 mg/min; hold for hypotension, QRS widening >50%, or QT prolongation. One RCT found procainamide superior to amiodarone for termination of stable VT[1]
- Amiodarone: 150 mg IV over 10 min, then 1 mg/min × 6 hrs, then 0.5 mg/min × 18 hrs
- Sotalol: IV formulation; avoid in decompensated HF or prolonged QT
Cardioversion
- Synchronized DC cardioversion is the most efficacious treatment at any point and should be performed if pharmacologic therapy fails or the patient deteriorates
- Requires procedural sedation (propofol, etomidate, or midazolam)
Idiopathic VT (no structural heart disease)
- RVOT VT: May respond to IV beta-blockers or adenosine
- Fascicular VT (verapamil-sensitive): May respond to IV verapamil — but only if this specific diagnosis is made with confidence by an arrhythmia expert
Long-term management
- ICD evaluation for secondary prevention in structural heart disease
- Antiarrhythmic therapy (amiodarone, sotalol, mexiletine) for recurrence prevention
- Catheter ablation for recurrent VT or VT storm[5]
- Optimize heart failure therapy (beta-blockers, ACEi/ARB, SGLT2i)
17. Disposition
All patients with sustained VT require admission
- ICU/CCU admission: New-onset VT, structural heart disease, reduced EF, recurrent episodes, required cardioversion, hemodynamic instability at any point
- Telemetry admission: Stable idiopathic VT in a young patient without structural heart disease after successful termination, pending further workup
- Electrophysiology consultation: All patients with sustained VT should have cardiology/EP consultation[2][4]
- Cardiology consultation triggers: New diagnosis of VT, VT storm, ICD evaluation, consideration for catheter ablation
- There is essentially no scenario in which a patient with documented sustained VT is discharged from the ED without inpatient evaluation.
18. Follow Up / Return Precautions
Post-discharge follow-up
- Cardiology/EP follow-up within 1–2 weeks of discharge
- ICD check within 1 week if newly implanted
- Repeat echocardiography if new structural findings
- Medication titration and monitoring (amiodarone requires thyroid, liver, and pulmonary function monitoring)
- Cardiac MRI if not completed during admission
- Return precautions — counsel patients to seek immediate care for:
- Recurrent palpitations, rapid heartbeat, or "fluttering"
- Lightheadedness, dizziness, or syncope
- Chest pain or shortness of breath
- ICD shocks (single shock → call clinic; multiple shocks → ED)
Expected recovery
- Idiopathic VT: Excellent prognosis with ablation (>90% success rate)[4]
- Structural heart disease VT: Chronic management required; >40% recurrence at 2 years without definitive therapy; ICD significantly reduces sudden death risk[4][11]
References
1. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
2. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
3. Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association. — Tisdale JE, Chung MK, Campbell KB, et al. Circulation. 2020.
4. Ventricular Arrhythmias and Sudden Cardiac Death. — John RM, Tedrow UB, Koplan BA, et al. Lancet. 2012.
5. Catheter Ablation of Ventricular Arrhythmias. — Shivkumar K. The New England Journal of Medicine. 2019.
6. Electrolyte Abnormalities in Patients Presenting With Ventricular Arrhythmia (From the LYTE-VT Study). — Laslett DB, Cooper JM, Greenberg RM, et al. The American Journal of Cardiology. 2020.
7. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Wigginton JG, Agarwal S, Bartos JA, et al. Circulation. 2025.
8. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). — European Heart Rhythm Association, Heart Rhythm Society, Zipes DP, et al. Journal of the American College of Cardiology. 2006.
9. Best Clinical Practice: Emergency Medicine Management of Stable Monomorphic Ventricular Tachycardia. — Long B, Koyfman A. The Journal of Emergency Medicine. 2017.
10. 2024 HRS Expert Consensus Statement on Arrhythmias in the Athlete: Evaluation, Treatment, and Return to Play. — Lampert R, Chung EH, Ackerman MJ, et al. Heart Rhythm. 2024.
11. Ventricular Tachycardia and Sudden Cardiac Death. — Koplan BA, Stevenson WG. Mayo Clinic Proceedings. 2009.
12. 2021 ACC/AHA Key Data Elements and Definitions for Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Heart Failure). — Bozkurt B, Hershberger RE, Butler J, et al. Journal of the American College of Cardiology. 2021.
13. 2019 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on Catheter Ablation of Ventricular Arrhythmias. — Cronin EM, Bogun FM, Maury P, et al. Heart Rhythm. 2020.
14. Sudden Death in Patients Without Structural Heart Disease. — Wever EF, Robles de Medina EO. Journal of the American College of Cardiology. 2004.
15. Ventricular Arrhythmias in the Absence of Structural Heart Disease. — Prystowsky EN, Padanilam BJ, Joshi S, Fogel RI. Journal of the American College of Cardiology. 2012.
16. Diagnostic evaluation of unexplained ventricular tachyarrhythmias in younger adults. — William J, Xiao X, Shirwaiker A, et al. Journal of Cardiovascular Electrophysiology. 2023.
17. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Panchal AR, Bartos JA, Cabañas JG, et al. Circulation. 2020.
18. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Heart Rhythm. 2018.
19. Approach to Narrow and Wide QRS Complex Tachyarrhythmias. — Elias Hanna Practical Cardiovascular Medicine 2e. 2022.