Ventricular Tachycardia (Unstable)
Unstable Ventricular Tachycardia (VT)
Unstable Ventricular Tachycardia (VT)
Unstable VT is a life-threatening emergency requiring immediate synchronized cardioversion (for monomorphic VT) or unsynchronized defibrillation (for polymorphic VT/VF).[1-3] Hemodynamic instability is defined by SBP <80 mmHg, altered mentation, syncope, chest pain, or signs of acute heart failure.[2] Any wide-complex tachycardia of unclear origin should be presumed to be VT.[1][4]
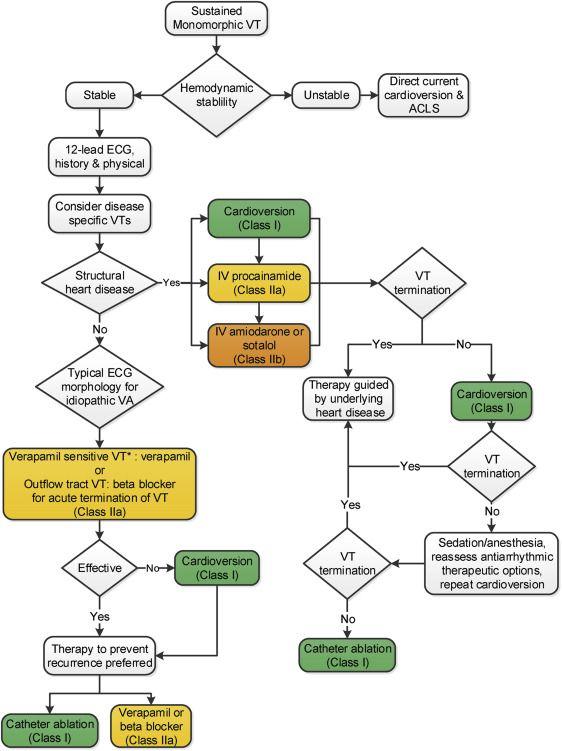
The following figure from the 2017 AHA/ACC/HRS Guidelines illustrates the acute management algorithm for sustained monomorphic VT, with the immediate pathway to cardioversion for unstable patients:
View full figure Figure 2. Management of Sustained Monomorphic VT 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. October 1, 2018.
1. History
- Key HPI questions: Onset (sudden vs. gradual), duration, associated symptoms (palpitations, chest pain, dyspnea, lightheadedness, syncope, near-syncope)
- Symptom characterization: Pounding in chest, "racing heart," sense of impending doom; may present with cardiac arrest
- Timing/triggers: Exertion, emotional stress, recent medication changes, illicit drug use (cocaine, methamphetamine), caffeine
- Severity/progression: Sustained (>30 seconds) vs. nonsustained; prior episodes; prior ICD shocks
- Associated symptoms: Diaphoresis, nausea, dyspnea, altered consciousness, seizure-like activity (from hypoperfusion)
- Important negatives: No preceding trauma, no recent surgery, no known ingestion
2. Alarm Features
- Pulselessness → treat as cardiac arrest (CPR + defibrillation per ACLS)[1][5]
- SBP <80 mmHg or altered mentation → immediate synchronized cardioversion[2]
- Polymorphic VT → always considered hemodynamically and electrically unstable; requires unsynchronized defibrillation at maximum energy[2][6]
- VT storm (≥3 episodes in 24 hours) → escalate to combination antiarrhythmics, IV beta-blockers, sedation, consider catheter ablation[7]
- Signs of acute MI (ST elevation, chest pain) → emergent coronary angiography[1][5]
- Torsades de Pointes (polymorphic VT with prolonged QT) → IV magnesium, overdrive pacing; avoid further QT-prolonging agents[2]
3. Medications
Acute Treatment (post-cardioversion or refractory VT)
- Amiodarone 150 mg IV over 10 min, then 1 mg/min × 6 hrs, then 0.5 mg/min × 18 hrs — Class I for hemodynamically unstable VT refractory to cardioversion[1][4]
- Lidocaine 1–1.5 mg/kg IV bolus, then 1–4 mg/min infusion — alternative, especially in acute MI setting[4-5]
- Procainamide 20–50 mg/min IV (max 17 mg/kg) — preferred for stable VT; use with caution in unstable patients due to hypotension risk[2][5]
- IV beta-blockers (esmolol) — particularly useful for polymorphic VT storm and ischemia-related VT[4][7]
Contraindicated medications
- Verapamil/diltiazem — absolutely contraindicated in wide-complex tachycardia of unknown origin; can cause profound hypotension, shock, and cardiac arrest[2][4]
- QT-prolonging agents in the setting of Torsades de Pointes[2]
- Avoid co-administration of multiple antiarrhythmics (arrhythmogenic risk)[2]
Medication contributors to VT
- Digitalis toxicity, Class IC antiarrhythmics (flecainide, propafenone), QT-prolonging drugs (sotalol, dofetilide, certain antibiotics/antipsychotics), cocaine, methamphetamine[3][8-9]
4. Diet
- Not directly applicable in the acute setting
- Electrolyte repletion is critical: Maintain K⁺ >4.0 mEq/L and Mg²⁺ >2.0 mg/dL to reduce arrhythmia recurrence[2][4]
- Long-term: Limit caffeine and alcohol; avoid stimulant-containing supplements
5. Review of Systems
- Cardiovascular: Chest pain, palpitations, syncope/presyncope, dyspnea on exertion, orthopnea, lower extremity edema
- Neurologic: Altered consciousness, seizure-like activity, focal deficits (post-arrest)
- Pulmonary: Dyspnea, cough (pulmonary edema from cardiogenic shock)
- GI: Nausea, abdominal pain (low-flow state)
- Psychiatric: Anxiety, sense of impending doom
6. Collateral History and Family History
- Collateral: Witnessed collapse? Duration of unresponsiveness? Bystander CPR? ICD in place? Recent medication changes?
- Family history: Sudden cardiac death (especially <40 years), cardiomyopathy (HCM, DCM, ARVC), channelopathies (Long QT, Brugada, CPVT)[10-11]
- Social context: Cocaine/stimulant use, anabolic steroids, energy drink consumption
7. Risk Factors
- Prior MI / ischemic cardiomyopathy — most common cause of sustained monomorphic VT (scar-related reentry)[3][12-13]
- Reduced LVEF (<35%) — strongest predictor of VT and sudden cardiac death[3][13]
- Nonischemic cardiomyopathy (DCM, HCM, ARVC, sarcoidosis)[3][12]
- Channelopathies: Long QT syndrome, Brugada syndrome, CPVT[10-11]
- Electrolyte abnormalities: Hypokalemia, hypomagnesemia, hypocalcemia[3-4]
- Acute coronary syndrome — most common cause of polymorphic VT/VF[12]
- Drug-induced proarrhythmia and QT prolongation[3][8]
- Heart failure, LVH, prior cardiac surgery[3][14]
8. Differential Diagnosis
- SVT with aberrant conduction (bundle branch block) — most important mimic; AV dissociation, fusion beats, and concordance favor VT[15-16]
- Pre-excited tachycardia (antidromic AVRT via accessory pathway)[15]
- Atrial flutter with 1:1 conduction and aberrancy — can closely mimic VT[17]
- Pacemaker-mediated tachycardia[6][18]
- ECG artifact mimicking VT[12]
- Polymorphic VT vs. VF — may be difficult to distinguish initially; both require defibrillation[2]
- Torsades de Pointes — specific subtype of polymorphic VT with QT prolongation; requires distinct treatment (magnesium, overdrive pacing)[2][6]
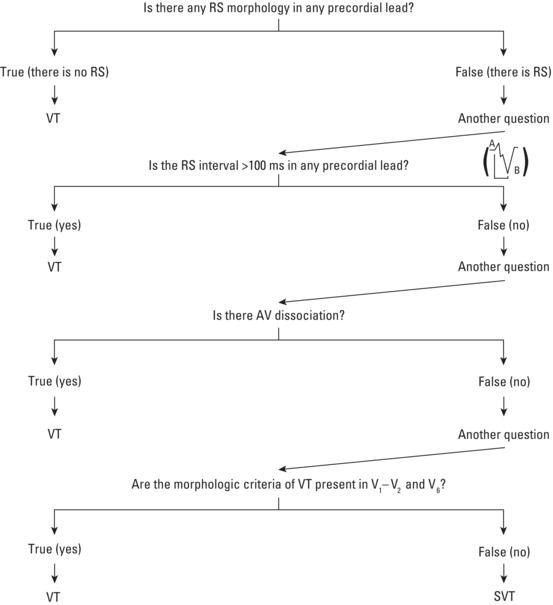
Key distinguishing ECG criteria (Brugada criteria)
- Absence of RS complex in all precordial leads → VT
- RS interval >100 ms in any precordial lead → VT
- AV dissociation → VT
- Morphologic criteria for VT in V1–V2 and V6 → VT
- The Brugada algorithm for differentiating VT from SVT is shown below:
View full figure Figure 16. Algorithm for the diagnosis of wide QRS tachycardia. When an RS complex is not visible in any precordial lead, we can make a diagnosis of ventricular tachycardia (VT). When an RS complex is present in one or more precordial leads, the longest RS interval should be measured (from start of the R wave to S wave nadir—see inside the figure). If the RS interval is greater than 100 ms, we can make a diagnosis of VT. If the interval is shorter, the next step is to check the presence of atrioventricular (AV) dissociation. If it is present, we can make a diagnosis of VT. If not present, the morphologic criteria for the differential diagnosis of VT should be checked in V1 and V6 leads. According to these, we will diagnose VT or supraventricular tachycardia ( Modified from Brugada et al . ). Read more Active Ventricular Arrhythmias. Clinical Electrocardiography. December 31, 2020.
9. Past Medical History
- Prior MI, coronary artery disease, PCI/CABG
- Known cardiomyopathy (ischemic, nonischemic, ARVC, HCM)
- Prior VT/VF episodes, cardiac arrest
- ICD or pacemaker in place (check device interrogation)
- Prior cardiac surgery (e.g., tetralogy of Fallot repair)
- Chronic kidney disease (electrolyte derangements)
- Thyroid disease
- Known channelopathy or family history of sudden death
10. Physical Exam
Vital sign abnormalities
- Hypotension (SBP <90 mmHg), tachycardia (rate typically 150–250 bpm), tachypnea, hypoxia
Focused exam
- General: Altered mental status, diaphoresis, pallor, cyanosis
- Neck: Cannon A waves (AV dissociation — pathognomonic for VT), JVD
- Cardiac: Rapid regular rhythm, variable S1 intensity (AV dissociation), S3 gallop (heart failure), murmurs (structural disease)
- Lungs: Crackles/rales (pulmonary edema from cardiogenic shock)
- Extremities: Cool, mottled, delayed capillary refill (poor perfusion)
- Neurologic: Level of consciousness, pupil reactivity (post-arrest)
11. Lab Studies
- Stat labs: BMP (K⁺, Mg²⁺, Ca²⁺, creatinine), troponin, CBC, lactate, ABG/VBG
- Expected abnormalities: Hypokalemia, hypomagnesemia, elevated troponin (ischemia or demand), lactic acidosis (hypoperfusion)
- Rule-out labs: TSH, drug levels (digoxin if applicable), urine drug screen (cocaine, amphetamines)
- Monitoring: Serial troponins, repeat BMP for electrolyte correction, coagulation studies if considering catheterization
12. Imaging
- Bedside echocardiography (first-line) — assess LVEF, wall motion abnormalities, structural heart disease, pericardial effusion[3]
- Chest X-ray — cardiomegaly, pulmonary edema, device lead positioning
- Coronary angiography — emergent if acute MI suspected (ST elevation or high clinical suspicion)[1][5]
- Cardiac MRI — post-stabilization for myocardial scar characterization, ARVC evaluation, sarcoidosis[3]
- CT coronary angiography — select patients for coronary evaluation when catheterization is not immediately indicated[3]
13. Special Tests
- 12-lead ECG during tachycardia (if obtainable before cardioversion) and after conversion — compare QRS morphology[3][16]
- Brugada criteria / Vereckei algorithm for VT vs. SVT differentiation[15][19]
- ICD/pacemaker interrogation — review stored electrograms, device programming[4]
- Electrophysiology study — post-stabilization for definitive diagnosis, risk stratification, and potential catheter ablation[12]
- Point-of-care ultrasound — rapid cardiac assessment, IVC for volume status
14. ECG
- Indications: Obtain on every patient; 12-lead during tachycardia is invaluable for diagnosis
Key ECG findings in VT
- Wide QRS (≥120 ms), regular rate 150–250 bpm[6]
- AV dissociation — most specific finding for VT[15]
- Fusion and capture beats — diagnostic of VT
- Concordance — all precordial QRS complexes positive or negative[15]
- Northwest axis (positive aVR, negative I and aVF) — strongly suggests VT[17]
- QRS >140 ms with RBBB pattern or >160 ms with LBBB pattern favors VT[16]
Dangerous ECG patterns
- Polymorphic VT — continuously changing QRS morphology; consider ischemia or channelopathy[12]
- Torsades de Pointes — waxing/waning QRS amplitude ("spindle" pattern) with prolonged QT[12]
- ST elevation during or after conversion — acute MI requiring emergent intervention[1]
- Brugada pattern (coved ST elevation V1–V3) — risk of VF[10]
15. Assessment
- Clinical summary: Unstable VT is a medical emergency with high mortality if untreated. The most common etiology is scar-related reentry from prior MI or structural heart disease.[3][13] Polymorphic VT is always considered unstable and often degenerates to VF.[2]
Severity stratification
- Pulseless VT → cardiac arrest protocol (CPR + defibrillation)
- VT with pulse but hemodynamically unstable → immediate synchronized cardioversion[1-2]
- VT storm (≥3 episodes/24 hrs) → ICU admission, combination therapy, consider ablation[7]
Typical vs. atypical presentations
- Typical: Sudden palpitations, presyncope/syncope, chest pain, dyspnea in a patient with known heart disease
- Atypical: Seizure-like activity (from cerebral hypoperfusion), abdominal pain, isolated altered mental status
- Complications: Cardiogenic shock, cardiac arrest, end-organ damage (renal, hepatic, neurologic), post-resuscitation syndrome
16. Treatment Plan
Initial stabilization (seconds to minutes)
- Pulseless VT → CPR, unsynchronized defibrillation (biphasic 120–200 J), follow ACLS algorithm[1]
- VT with pulse, hemodynamically unstable → immediate synchronized cardioversion (biphasic 100 J, escalate as needed); procedural sedation if patient is conscious and time permits[1-2][4]
- Monomorphic VT → synchronized cardioversion; Polymorphic VT → unsynchronized defibrillation at maximum energy[2][6]
Post-cardioversion / refractory VT
- IV amiodarone 150 mg over 10 min → 1 mg/min infusion (Class I for recurrent unstable VT)[1][4]
- IV lidocaine 1–1.5 mg/kg bolus → 1–4 mg/min (especially in acute MI)[4-5]
- IV esmolol for sympathetically mediated or ischemia-related VT storm[7]
- Correct K⁺ to >4.0 mEq/L and Mg²⁺ to >2.0 mg/dL[2][4]
For Torsades de Pointes specifically
- IV magnesium 2 g bolus[2][6]
- Overdrive pacing or isoproterenol for bradycardia/pause-dependent TdP[2]
- Discontinue all QT-prolonging agents[2]
For VT storm refractory to initial therapy
- Combination amiodarone + IV beta-blocker (esmolol preferred)
- Sedation with dexmedetomidine or benzodiazepines
- Stellate ganglion block
- Deep sedation/general anesthesia
- Catheter ablation for incessant VT
- Mechanical circulatory support (IABP, VA-ECMO) for cardiogenic shock
Definitive management (post-stabilization)
- ICD evaluation for secondary prevention of sudden cardiac death[3][12]
- Catheter ablation for recurrent VT[3]
- Coronary revascularization if ischemia-driven[1][5]
17. Disposition
- Admission criteria (all unstable VT patients require admission):
- ICU/CCU admission for all hemodynamically unstable VT, VT storm, post-cardiac arrest, or ongoing antiarrhythmic infusions[7]
- Telemetry/step-down for patients who convert and remain stable with identified and corrected reversible cause
- Discharge criteria: Unstable VT patients are never discharged from the ED
Specialist consultation triggers
- Cardiology — all patients with sustained VT
- Electrophysiology — VT storm, recurrent VT, ICD evaluation, catheter ablation candidacy[7][12]
- Interventional cardiology — suspected acute coronary syndrome[1][5]
- Cardiac surgery — if CABG indicated or mechanical circulatory support needed
18. Follow Up / Return Precautions
Inpatient follow-up
- Continuous telemetry monitoring for ≥48 hours post-conversion
- Serial troponins and electrolyte monitoring
- Echocardiography for LVEF assessment if not already obtained[3]
- Cardiac MRI for scar characterization when appropriate[3]
- EP consultation for ICD implantation and/or ablation planning[3][12]
Post-discharge (after inpatient stabilization)
- Cardiology/EP follow-up within 1–2 weeks
- ICD follow-up and device checks
- Medication reconciliation — ensure no QT-prolonging agents, optimize heart failure therapy
- Avoid driving per local regulations (typically restricted for 6 months post-VT/VF event)
Symptoms requiring immediate reassessment
- Recurrent palpitations, presyncope, syncope
- ICD shocks (single or multiple)
- Chest pain, worsening dyspnea
- Any loss of consciousness
- Expected recovery course: Depends on underlying etiology. Patients with reversible causes (electrolyte abnormalities, drug-induced) have favorable prognosis if the cause is corrected. Patients with structural heart disease and recurrent VT have >40% recurrence within 2 years and require long-term ICD and antiarrhythmic management.[12]
References
1. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
2. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Wigginton JG, Agarwal S, Bartos JA, et al. Circulation. 2025.
3. Catheter Ablation of Ventricular Arrhythmias. — Shivkumar K. The New England Journal of Medicine. 2019.
4. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). — European Heart Rhythm Association, Heart Rhythm Society, Zipes DP, et al. Journal of the American College of Cardiology. 2006.
5. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Heart Rhythm. 2018.
6. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Panchal AR, Bartos JA, Cabañas JG, et al. Circulation. 2020.
7. Multidisciplinary Critical Care Management of Electrical Storm: JACC State-of-the-Art Review. — Jentzer JC, Noseworthy PA, Kashou AH, et al. Journal of the American College of Cardiology. 2023.
8. Palpitations: Evaluation, Management, and Wearable Smart Devices. — Gauer RL, Thomas MF, McNutt RA. American Family Physician. 2024.
9. ECG Clues for Diagnosing Ventricular Tachycardia Mechanism. — Riley MP, Marchlinski FE. Journal of Cardiovascular Electrophysiology. 2008.
10. 2021 ACC/AHA Key Data Elements and Definitions for Heart Failure: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Data Standards (Writing Committee to Develop Clinical Data Standards for Heart Failure). — Bozkurt B, Hershberger RE, Butler J, et al. Journal of the American College of Cardiology. 2021.
11. 2024 HRS Expert Consensus Statement on Arrhythmias in the Athlete: Evaluation, Treatment, and Return to Play. — Lampert R, Chung EH, Ackerman MJ, et al. Heart Rhythm. 2024.
12. Ventricular Arrhythmias and Sudden Cardiac Death. — John RM, Tedrow UB, Koplan BA, et al. Lancet. 2012.
13. Ventricular Tachycardia and Sudden Cardiac Death. — Koplan BA, Stevenson WG. Mayo Clinic Proceedings. 2009.
14. Cardiac arrhythmias in arterial hypertension. — Varvarousis D, Kallistratos M, Poulimenos L, et al. Journal of Clinical Hypertension. 2020.
15. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Page RL, Joglar JA, Caldwell MA, et al. Journal of the American College of Cardiology. 2016.
16. 2019 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on Catheter Ablation of Ventricular Arrhythmias. — Cronin EM, Bogun FM, Maury P, et al. Heart Rhythm. 2020.
17. Changing Rapid Wide Complex Tachycardia in a Middle-Aged Man. — Ramakumar V, Gupta A, Jain A. JAMA Internal Medicine. 2025.
18. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
19. Common Types of Supraventricular Tachycardia: Diagnosis and Management. — Nasir M, Sturts A, Sturts A. American Family Physician. 2023.
20. Active Ventricular Arrhythmias. — Antoni Bayés De Luna, Miquel Fiol‐Sala, Antoni Bayés‐Genís, et al. Clinical Electrocardiography. 2021.