Vestibular Neuronitis
Vestibular neuritis is the second most common cause of peripheral vestibular vertigo, caused by presumed viral inflammation (most likely HSV-1 reactivation) of the vestibular portion of CN VIII. It…
Vestibular neuritis is the second most common cause of peripheral vestibular vertigo, caused by presumed viral inflammation (most likely HSV-1 reactivation) of the vestibular portion of CN VIII. It presents as acute, sustained rotatory vertigo lasting days, with nausea, vomiting, and gait instability, but without hearing loss or focal neurologic deficits. Annual incidence is approximately 3.5 per 100,000, most commonly affecting patients aged 30–50 years.[1-4]
1. History
- Onset and duration: Sudden onset of severe, continuous rotatory vertigo lasting hours to days (not seconds/minutes); maximal within minutes to hours[5-6]
- Preceding illness: Viral prodrome (URI) in days to weeks prior is common[7-8]
- Character: True spinning sensation (room spinning or self-spinning), not lightheadedness or presyncope
- Aggravating factors: Worsened by head movement; not triggered by positional changes (unlike BPPV)
- Associated symptoms: Severe nausea, vomiting, oscillopsia (visual illusion of movement), gait unsteadiness[2][8]
- Important negatives: No hearing loss, no tinnitus, no aural fullness, no diplopia, no dysarthria, no dysphagia, no limb weakness/numbness, no headache[2][7]
- Temporal course: Acute vertigo lasts 1–3 days, then progressively improves; residual imbalance may persist weeks to months[1][7]
2. Alarm Features
- "Deadly Ds" suggesting central etiology (stroke): Diplopia, dysarthria, dysphagia, dysphonia, dysmetria, dysesthesia[9]
- Negative head impulse test (normal VOR) — suggests central lesion, not vestibular neuritis[2][9]
- Direction-changing nystagmus or vertical/pure torsional nystagmus — central pattern[10]
- Skew deviation (vertical misalignment on alternate cover test) — central sign[9][11]
- Severe truncal ataxia with inability to stand or walk independently — consider posterior fossa stroke even with "peripheral-appearing" nystagmus[9]
- Unprecedented severe headache or neck stiffness[2]
- No improvement within 1–2 days — reconsider diagnosis[2]
- New hearing loss — suggests labyrinthitis, AICA stroke, or Ménière disease[7][12]
- Vascular risk factors (HTN, DM, atrial fibrillation, age >60) in the setting of AVS increase stroke probability[9][13]
3. Medications
Acute symptomatic treatment (limit to 3–5 days maximum)
- Promethazine 25 mg IM/IV — first-line for acute severe vomiting[5]
- Prochlorperazine 10 mg IM/IV — add if vomiting persists[5]
- Ondansetron 4 mg IV — antiemetic alternative
- Meclizine 25 mg PO q6–8h — oral vestibular suppressant once tolerating PO[5][9]
- Dimenhydrinate 50 mg PO q6–8h — alternative oral suppressant[5]
- Benzodiazepines (diazepam 5 mg, lorazepam 0.5–1 mg) — for refractory cases; use sparingly[1]
Key cautions
- All vestibular suppressants (antihistamines, antiemetics, benzodiazepines) block central compensation — discontinue as soon as possible, no longer than 3–5 days[1][9][14]
- Antivirals (valacyclovir, acyclovir) are not effective and not recommended[1][4]
- Corticosteroids: Controversial; GRACE-3 guidelines suggest shared decision-making for patients presenting within 3 days of onset (conditional recommendation, very low certainty evidence). Consider methylprednisolone taper or prednisone if used. Avoid in poorly controlled diabetes or bipolar disorder[9][15]
4. Diet
- Hydration is critical — patients often become dehydrated from vomiting; IV fluids may be needed acutely
- Small, bland meals during the acute phase to minimize nausea
- No specific long-term dietary restrictions
- Avoid alcohol during the acute and early recovery phase (worsens vestibular symptoms)
5. Review of Systems
- Neurologic: Headache, vision changes, diplopia, facial weakness/numbness, limb weakness, sensory changes, speech difficulty, swallowing difficulty
- Otologic: Hearing loss, tinnitus, aural fullness, ear pain, otorrhea (vesicular rash → Ramsay Hunt)[16]
- Cardiovascular: Palpitations, syncope, presyncope (to exclude cardiogenic vertigo)[1][17]
- Psychiatric: Anxiety, panic symptoms (can mimic or coexist with vestibular disorders)
- Constitutional: Fever, recent URI, weight loss
6. Collateral History and Family History
- Collateral: Witnesses can describe nystagmus direction, gait deviation, level of consciousness, and symptom onset (hyperacute onset more concerning for vascular etiology)[12]
- Medication list: Ototoxic drugs (aminoglycosides, loop diuretics, cisplatin)
- Family history: Migraine (vestibular migraine is a key differential), Ménière disease, stroke risk factors
- Social context: Occupational hazards (driving, operating machinery), fall risk at home, ability to tolerate PO
7. Risk Factors
- Recent viral illness (URI) — most commonly cited precipitant[8]
- Age 30–50 years — peak incidence[1]
- HSV-1 latent infection of vestibular ganglia — reactivation theory[4][8]
- Seasonal variation — some evidence of clustering during viral epidemics[8]
- Vascular risk factors (HTN, DM, hyperlipidemia, smoking) — may contribute via microvascular mechanism; also raise concern for stroke as an alternative diagnosis[9][18]
- No strong hereditary predisposition identified
8. Differential Diagnosis
Cannot-miss diagnoses
- Posterior circulation stroke (cerebellar/brainstem infarction) — up to 25% of AVS presentations; may mimic vestibular neuritis with "peripheral-appearing" nystagmus in up to 28/44 stroke patients in one series[10-11][13]
- Labyrinthine infarction — hyperacute onset, no viral prodrome, hearing loss may be present; mimics vestibular neuritis on HINTS[12]
Important differentials
- Labyrinthitis — vestibular neuritis + hearing loss[6]
- Ménière disease — recurrent episodes, hearing loss, tinnitus, aural fullness[7]
- Vestibular migraine — episodic, migraine history, may lack nystagmus between attacks[7]
- Ramsay Hunt syndrome (HZO) — vesicular rash on ear, facial palsy, more severe vestibular loss[16]
- Cerebellopontine angle tumor (vestibular schwannoma) — insidious onset, hearing loss, facial palsy[7]
- Demyelinating disease (MS) — subacute, may have other CNS signs[7]
- BPPV — brief episodes (<1 min), positionally triggered, positive Dix-Hallpike[1]
9. Past Medical History
- Prior episodes of vertigo (recurrence is atypical for vestibular neuritis — consider Ménière or vestibular migraine)
- History of migraine
- Cerebrovascular disease or vascular risk factors
- Autoimmune conditions
- Prior ear surgery or ototoxic drug exposure
- Psychiatric history (anxiety/panic disorder can coexist)
- Some patients with vestibular neuritis subsequently develop BPPV[1]
10. Physical Exam
Vital signs
- Generally normal; check for hypertension (may suggest stroke), orthostatic hypotension, arrhythmia
HINTS exam (the critical bedside test in AVS)
- Head Impulse Test (HI): Positive (catch-up saccade toward affected side) = peripheral → supports vestibular neuritis. Negative HIT in AVS is concerning for central cause[2][9]
- Nystagmus (N): Unidirectional horizontal-torsional, fast phase beating away from the affected ear. Should not change direction with gaze. Direction-changing nystagmus = central[2][10]
- Test of Skew (TS): Negative (no vertical misalignment on alternate cover test). Positive skew = central[9]
- All three peripheral on HINTS → sensitivity >95% for ruling out stroke (superior to early MRI)[9][11]
Additional exam
- Romberg test: Falls toward the affected ear[8]
- Gait: Deviation/falling toward the affected side[1]
- Dix-Hallpike: Negative (does not trigger typical BPPV nystagmus)[1]
- Hearing: Grossly normal (finger rub, Weber/Rinne); hearing loss = labyrinthitis or central cause[2]
- Cranial nerves: Full exam to exclude focal deficits
- Cerebellar testing: Finger-to-nose, heel-to-shin — should be normal; dysmetria suggests central lesion[9]
11. Lab Studies
- Routine labs are generally not required for a classic presentation[19]
- Consider BMP if dehydrated from vomiting or if IV fluids are needed
- Glucose — to exclude hypoglycemia as a contributor
- CBC — if infection is suspected
- TSH — if chronic dizziness or atypical presentation
- RPR/FTA-ABS — if risk factors for syphilitic labyrinthitis
- Labs to rule out dangerous conditions: troponin only if cardiac symptoms present; routine troponin in dizzy patients is not recommended due to high false-positive rate[1]
12. Imaging
- No imaging is needed when HINTS is fully peripheral, hearing is normal, and the patient can stand unaided[9]
MRI with DWI (not CT): Indicated when
- Any central sign on HINTS[9]
- Inability to stand or walk independently[9]
- Vascular risk factors with diagnostic uncertainty
- No improvement within 48 hours[2]
- CT of the head is not recommended — sensitivity for posterior fossa stroke is very low (<50%)[13]
- CT angiography: Consider if vertebral artery dissection is suspected
- ACR Appropriateness Criteria: In isolated AVS with peripheral HINTS, imaging is usually not appropriate[13]
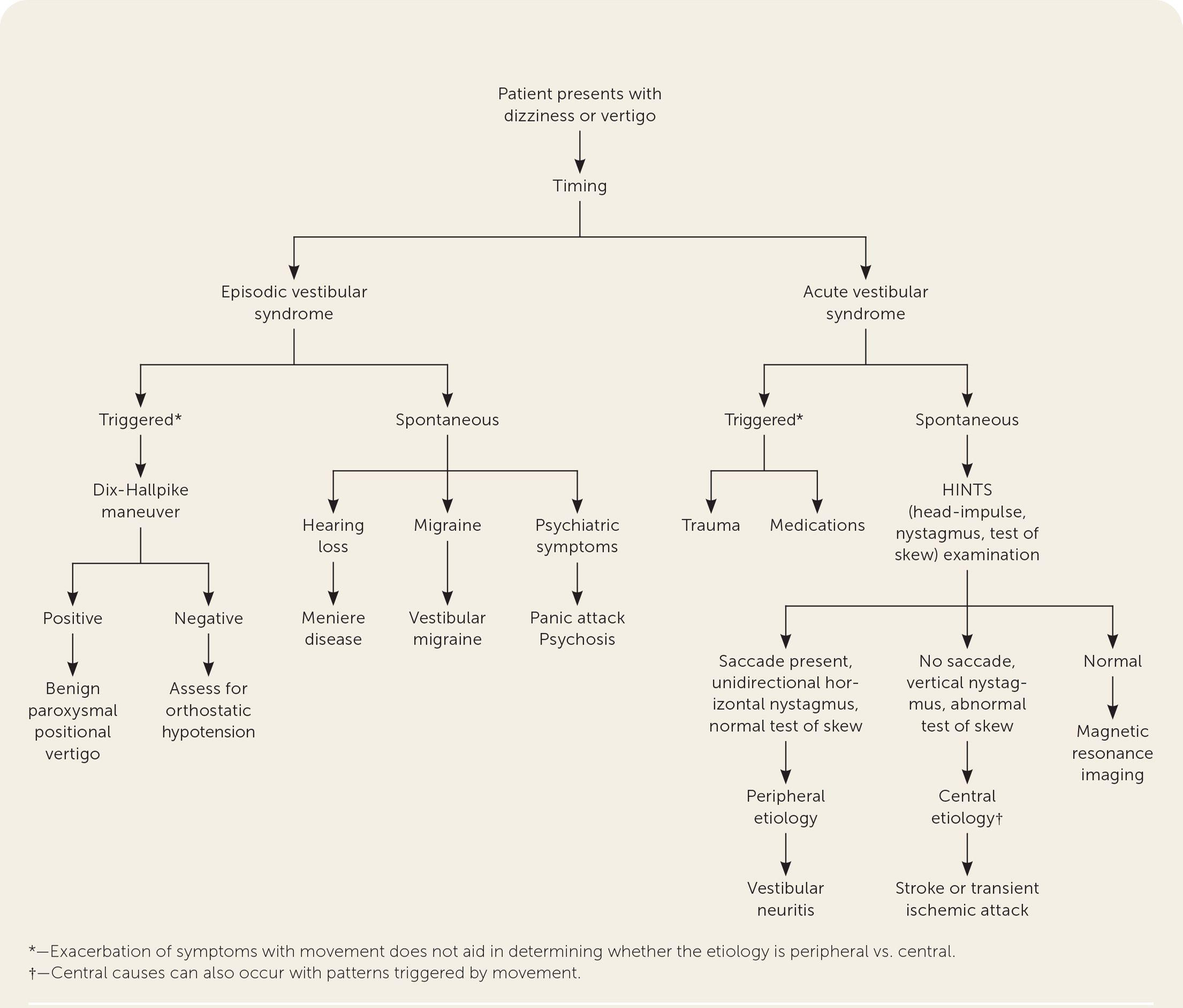
- The following diagnostic algorithm from the AAFP illustrates the TiTrATE approach to evaluating dizziness, including the role of HINTS in distinguishing vestibular neuritis from central causes:
- View full figure Figure 1. Diagnostic evaluation of dizziness. Adapted with permission from Muncie HL, Sirmans SM, James E. Dizziness: Approach to evaluation and management. Am Fam Physician. 2017;95(3):156. Dizziness: Evaluation and Management. Am Fam Physician. April 30, 2023.
13. Special Tests
- HINTS Plus: HINTS + hearing test (finger rub or audiometry) — adding hearing loss detection increases sensitivity for AICA stroke[9]
- Caloric testing: Demonstrates ipsilateral canal paresis; rarely needed acutely but confirms diagnosis[4][8]
- Video head impulse test (vHIT): Quantitative VOR gain measurement; gain ≤0.68 highly sensitive for vestibular neuritis vs. stroke[20-21]
- VEMPs (vestibular evoked myogenic potentials): Assess otolith function; abnormal oVEMP asymmetry ratio is specific for vestibular neuritis[20-21]
- Subjective visual horizontal (SVH): Deviation >2.5° toward affected side in 97.6% of vestibular neuritis[20]
- Videonystagmography (VNG): Formal nystagmus recording; useful for follow-up
14. ECG
- Not routinely indicated for classic vestibular neuritis presentation
- Obtain ECG if: Palpitations, syncope/presyncope, irregular pulse, significant bradycardia or tachycardia, or suspicion of cardiogenic dizziness[1][9]
- Arrhythmias to consider: Atrial fibrillation (also a stroke risk factor), bradyarrhythmias, prolonged QTc (if using ondansetron or promethazine)
- If episodic dizziness with palpitations, consider Holter or event monitoring[17]
15. Assessment
Clinical summary: Vestibular neuritis is a clinical diagnosis based on acute, sustained rotatory vertigo with peripheral HINTS findings, no hearing loss, and no focal neurologic deficits.[1-2][5] It is a self-limiting condition with the acute phase lasting 1–3 days, followed by gradual improvement over weeks. However, up to 50% of patients may develop persistent symptoms including imbalance or motion sensitivity.[7]
Severity stratification
- Mild: Ambulatory, tolerating PO, minimal nausea → outpatient management
- Moderate: Significant nausea/vomiting, unsteady gait but can stand → ED treatment, likely discharge
- Severe: Intractable vomiting, unable to stand, dehydration → consider observation/admission
Complications
- Secondary BPPV (common)[1]
- Chronic vestibular hypofunction with persistent imbalance
- Anxiety/depression related to chronic dizziness[22]
- Incomplete peripheral vestibular recovery (~80% still have caloric paresis at 6 months)[4]
16. Treatment Plan
Initial stabilization (ED)
- IV fluids for dehydration
- Promethazine 25 mg IM or ondansetron 4 mg IV for acute nausea/vomiting[5]
- Prochlorperazine 10 mg IM/IV if refractory[5]
- Reassurance and explanation of expected disease course
Outpatient medications (short-term only, ≤3–5 days)
- Meclizine 25 mg PO q6–8h PRN or dimenhydrinate 50 mg PO q6–8h PRN[5][9]
- Discontinue vestibular suppressants as soon as tolerable to allow central compensation[1][9][14]
Corticosteroids (shared decision-making)
- If within 3 days of onset: consider methylprednisolone starting at 100 mg daily, tapered over ~3 weeks, or prednisone equivalent taper[4][9]
- Evidence shows improved caloric recovery but uncertain symptomatic benefit[15]
Vestibular rehabilitation therapy (VRT)
- Refer all patients regardless of steroid use[9][23]
- Start once acute nausea/vomiting resolves[5]
- Earlier initiation (within 1–2 weeks) associated with better outcomes[14]
- Exercises include VOR adaptation (VORx1), gaze stabilization, balance training, and habituation exercises[14]
- Moderate-to-strong evidence supporting efficacy for symptom reduction, balance, gait, and quality of life[23]
- Statistically significant improvement in perceived dizziness at 3 and 12 months with early VRT[22]
17. Disposition
Discharge criteria (majority of patients)
- Peripheral HINTS exam with no central features[9]
- Able to stand and ambulate (even if unsteady)[9]
- Tolerating oral fluids and medications
- Adequate home support and follow-up arranged
Admission/observation criteria
- Intractable vomiting with inability to tolerate PO
- Severe dehydration requiring ongoing IV fluids
- Inability to stand or walk independently (even with peripheral HINTS — MRI needed)[9]
- Any central signs on HINTS or neurologic exam → stroke workup
- Diagnostic uncertainty in patients with high vascular risk
Specialist consultation triggers
- Neurology: Any concern for central etiology, atypical features, or failure to improve
- ENT/Neurotology: Hearing loss, recurrent episodes, suspected Ménière disease
- Physical therapy (vestibular specialist): All patients for VRT[9]
18. Follow Up / Return Precautions
Follow-up timing
- Primary care or ENT follow-up within 1–2 weeks
- Vestibular rehabilitation referral at discharge[9]
- Return precautions — instruct patients to return immediately for:
- New headache, vision changes, or double vision
- Slurred speech, facial droop, or limb weakness/numbness
- Worsening vertigo after initial improvement
- Inability to keep down fluids
- New hearing loss or ear pain
- Falls or inability to walk
Patient counseling
- Vertigo is expected to improve significantly within 2–3 days, with residual imbalance resolving over weeks to months[1][5]
- Avoid driving until vertigo resolves and balance is stable
- Vestibular exercises may initially provoke dizziness — this is expected and necessary for recovery[5]
- Avoid vestibular suppressant medications beyond 3–5 days[9]
- Some patients (~10–15%) may develop positional vertigo (BPPV) afterward — this is treatable[1]
- Vestibular exercises should be started when the acute stage of nausea and vomiting has ended. Many of the exercises will result in dizziness. This sensation is a necessary stimulus for compensation; antivertiginous medications should be avoided as much as possible in order to maximize the beneficial effect.
- — Robert W. Baloh, M.D., UCLA School of Medicine
- Vestibular Neuritis. N Engl J Med. March 12, 2003.
References
1. Dizziness: Evaluation and Management. — Rogers TS, Noel MA, Garcia B. American Family Physician. 2023.
2. Vestibular Neuritis. — Jeong SH, Kim HJ, Kim JS. Seminars in Neurology. 2013.
3. Vestibular Neuritis. — Strupp M, Brandt T. Seminars in Neurology. 2009.
4. Methylprednisolone, Valacyclovir, or the Combination for Vestibular Neuritis. — Strupp M, Zingler VC, Arbusow V, et al. The New England Journal of Medicine. 2004.
5. Vestibular Neuritis. — Baloh RW. The New England Journal of Medicine. 2003.
6. Clinical Reasoning: A 55-Year-Old Woman With Vertigo. A Dizzying Conundrum. — Gold DR, Reich SG. Neurology. 2012.
7. Clinical Reasoning: A 24-Year-Old Man With Persistent Spontaneous Dizziness. — Isaza-Pierotti DF, Sanchez JA, Kilgo WA. Neurology. 2025.
8. Corticosteroids for the Treatment of Idiopathic Acute Vestibular Dysfunction (Vestibular Neuritis). — Fishman JM, Burgess C, Waddell A. The Cochrane Database of Systematic Reviews. 2011.
9. Guidelines for Reasonable and Appropriate Care in the Emergency Department 3 (GRACE-3): Acute Dizziness and Vertigo in the Emergency Department. — Edlow JA, Carpenter C, Akhter M, et al. Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine. 2023.
10. Capturing Nystagmus in the Emergency Room: Posterior Circulation Stroke Versus Acute Vestibular Neuritis. — Nham B, Akdal G, Young AS, et al. Journal of Neurology. 2023.
11. Head Impulse, Nystagmus, and Test of Skew Examination for Diagnosing Central Causes of Acute Vestibular Syndrome. — Gottlieb M, Peksa GD, Carlson JN. The Cochrane Database of Systematic Reviews. 2023.
12. Pearls & Oy-Sters: Labyrinthine Infarction Mimicking Vestibular Neuritis. — Nam HW, Yoo D, Lee SU, et al. Neurology. 2021.
13. ACR Appropriateness Criteria® Dizziness and Ataxia: 2023 Update. — Wang LL, Thompson TA, Shih RY, et al. Journal of the American College of Radiology : JACR. 2024.
14. Vestibular Rehabilitation for Peripheral Vestibular Hypofunction: An Updated Clinical Practice Guideline From the Academy of Neurologic Physical Therapy of the American Physical Therapy Association. — Hall CD, Herdman SJ, Whitney SL, et al. Journal of Neurologic Physical Therapy : JNPT. 2022.
15. Corticosteroids for Patients With Vestibular Neuritis: An Evidence Synthesis for Guidelines for Reasonable and Appropriate Care in the Emergency Department. — Oliveira J E Silva L, Khoujah D, Naples JG, et al. Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine. 2023.
16. Vestibular Nucleus Involvement in Patients With Acute Vertigo Due to Herpes Zoster Oticus or Vestibular Neuritis. — Yacovino DA, Perez Akly MS, Ibañez T, Cherchi M. Neurology. 2023.
17. Wearable ECG Patch Monitoring for 72 h Is Comparable to Conventional Holter Monitoring for 24 h to Detect Cardiogenic Vertigo. — Kim HA, Lee H, Park HS, et al. Scientific Reports. 2025.
18. Clinical Features and Neurotologic Findings in Patients With Acute Unilateral Peripheral Vestibulopathy Associated With Antiganglioside Antibody. — Kim KT, Park E, Lee SU, et al. Neurology. 2023.
19. Dizziness: Approach to Evaluation and Management. — Muncie HL, Sirmans SM, James E. American Family Physician. 2017.
20. Modern Vestibular Tests Can Accurately Separate Stroke and Vestibular Neuritis. — Nham B, Wang C, Reid N, et al. Journal of Neurology. 2023.
21. Separating Posterior-Circulation Stroke From Vestibular Neuritis With Quantitative Vestibular Testing. — Calic Z, Nham B, Bradshaw AP, et al. Clinical Neurophysiology : Official Journal of the International Federation of Clinical Neurophysiology. 2020.
22. Efficacy of Vestibular Rehabilitation Following Acute Vestibular Neuritis: A Randomized Controlled Trial. — Tokle G, Mørkved S, Bråthen G, et al. Otology & Neurotology : Official Publication of the American Otological Society, American Neurotology Society European Academy of Otology and Neurotology. 2020.
23. Vestibular Rehabilitation for Unilateral Peripheral Vestibular Dysfunction. — McDonnell MN, Hillier SL. The Cochrane Database of Systematic Reviews. 2015.