Vitamin D Deficiency (Severe/Rickets)
Severe vitamin D deficiency (25-OHD <30 nmol/L or <12 ng/mL) causes rickets in children (defective growth plate mineralization) and osteomalacia in adults (defective bone matrix mineralization), wi…
Severe vitamin D deficiency (25-OHD <30 nmol/L or <12 ng/mL) causes rickets in children (defective growth plate mineralization) and osteomalacia in adults (defective bone matrix mineralization), with life-threatening complications including hypocalcemic seizures, dilated cardiomyopathy, and heart failure.[1-2]
1. History
- Key HPI: Bone pain location and duration, limb deformity progression, difficulty walking or waddling gait, delayed motor milestones, growth failure, muscle weakness, irritability, lethargy[3-4]
- Symptom characterization: Insidious onset; skeletal deformities worsen during periods of rapid growth (infancy, adolescence); adults present with vague diffuse musculoskeletal aches and proximal weakness[1][5]
- Timing/triggers: Symptoms peak between 3–18 months of age in children; winter months exacerbate deficiency due to reduced UV exposure[6]
- Associated symptoms: Seizures (may be the presenting symptom), tetany, recurrent respiratory infections, dental abnormalities, failure to thrive[6-7]
- Important negatives: Ask about dietary intake (exclusive breastfeeding without supplementation, vegan/restrictive diets), sun exposure habits, sunscreen use, geographic latitude[3][8]
2. Alarm Features
- Hypocalcemic seizures — may be focal or generalized tonic-clonic; incidence ~3.49/million children aged 0–15 years[6]
- Dilated cardiomyopathy / heart failure — especially in infants; presents with acute heart failure or cardiogenic shock[2]
- Laryngospasm and tetany[9]
- Prolonged QT interval → risk of torsades de pointes and ventricular arrhythmias[9-10]
- Pathologic fractures with minimal trauma[3]
- Craniotabes (soft skull bones) in neonates — suggests severe, prolonged deficiency[3-4]
3. Medications
Medications that cause/worsen vitamin D deficiency
- Anticonvulsants (phenobarbital, phenytoin, carbamazepine) — induce CYP3A4, accelerate vitamin D catabolism[13]
- Systemic glucocorticoids
- Rifampin, isoniazid
- Antiretrovirals (HAART)
- Cholestyramine, orlistat (impair absorption)
- Ketoconazole
Treatment medications
- Cholecalciferol (D3) or ergocalciferol (D2) — oral preferred[14]
- Calcium gluconate IV for acute symptomatic hypocalcemia[6][15]
- Oral calcium supplementation (calcium carbonate or citrate)[3]
- Contraindicated: Anticonvulsants should NOT be used for hypocalcemic seizures — some can worsen hypocalcemia; treat the calcium deficit instead[6]
- Caution: Narrow therapeutic-toxic window with high-dose vitamin D; monitor for hypercalcemia and hypercalciuria[16]
4. Diet
- Dietary triggers of deficiency: Exclusive breastfeeding without supplementation (breast milk contains only 15–50 IU/L vitamin D), vegan diets, dairy-free diets, low calcium intake[3][6][17]
- Dietary sources of vitamin D: Oily fish (salmon, mackerel), fortified milk, fortified cereals, egg yolks, liver, cod liver oil[3]
- Calcium-rich foods: Dairy products, fortified plant milks, leafy greens, tofu
- Acute management: Ensure adequate calcium intake ≥500 mg/day in children alongside vitamin D replacement[18]
- Long-term: Dietary counseling on vitamin D and calcium-rich foods; food fortification is the most cost-effective population strategy[1]
5. Review of Systems
- Musculoskeletal: Bone pain, limb deformity, difficulty walking, proximal weakness, fractures
- Neurological: Seizures, irritability, lethargy, paresthesias, muscle cramps/spasms[6-7][9]
- Cardiovascular: Dyspnea, poor feeding (infants with cardiomyopathy)[2]
- Growth/development: Short stature, delayed milestones, delayed dentition[3-4]
- GI: Assess for malabsorption symptoms (celiac disease, IBD, pancreatic insufficiency)
- Respiratory: Recurrent infections (associated with severe vitamin D deficiency in infancy)[6]
6. Collateral History and Family History
- Maternal history: Vitamin D status during pregnancy, dietary restrictions, sun exposure, supplementation practices[3]
- Family history: Consanguinity (raises suspicion for genetic rickets — VDDR types 1 and 2, X-linked hypophosphatemia)[4][19]
- Social context: Cultural practices (veiling, sun avoidance), immigration from low-latitude to high-latitude countries, socioeconomic status, food insecurity[1][6]
- Feeding history: Duration of exclusive breastfeeding, formula use (formula is fortified with ~400 IU/L), complementary food introduction[17]
7. Risk Factors
- Dark skin pigmentation — reduced cutaneous vitamin D synthesis[3][8]
- Exclusively breastfed infants without vitamin D supplementation[3][17]
- Limited sun exposure — indoor lifestyle, high latitude, winter season, sunscreen use, veiling[1][8]
- Maternal vitamin D deficiency during pregnancy[3]
- Obesity — vitamin D sequestered in adipose tissue[8]
- Malabsorption — celiac disease, IBD, cystic fibrosis, short bowel syndrome[12]
- Chronic kidney or liver disease — impaired vitamin D metabolism[20]
- Age <2 years and adolescence — periods of rapid growth[4][21]
- Medications — anticonvulsants, glucocorticoids, rifampin[11][13]
8. Differential Diagnosis
- Nutritional rickets (vitamin D and/or calcium deficiency) — most common cause worldwide[1][4]
- X-linked hypophosphatemia (XLH) — most common genetic cause; PHEX mutation, elevated FGF23, low phosphate, normal calcium[22-23]
- Vitamin D-dependent rickets type 1A (CYP27B1 mutation) — low calcitriol, responds to calcitriol replacement[19][23]
- Vitamin D-dependent rickets type 2 (VDR mutation) — end-organ resistance, often with alopecia[19][22]
- Hypophosphatasia — low ALP (distinguishing feature), ALPL mutation[22]
- Renal osteodystrophy — chronic kidney disease with impaired 1,25(OH)₂D production[20]
- Fanconi syndrome / renal tubular acidosis — phosphate wasting, metabolic acidosis[20]
- Tumor-induced osteomalacia — FGF23-secreting mesenchymal tumor (rare in children)[22]
- Non-accidental injury (child abuse) — must be considered in infants with fractures; rickets is a recognized differential[20]
9. Past Medical History
- Previous episodes of hypocalcemia or seizures
- Prematurity (reduced vitamin D stores)
- Chronic liver or kidney disease
- Celiac disease, IBD, or other malabsorptive conditions
- History of bariatric surgery (adults)
- Surgical history (gastrectomy, bowel resection)
- Medication history — especially anticonvulsants, steroids
10. Physical Exam
- Vital signs: Tachycardia, tachypnea (if heart failure present)
- Head: Craniotabes (ping-pong ball sensation on palpation of skull), frontal bossing, delayed fontanelle closure, dental enamel hypoplasia[3-4]
- Chest: Rachitic rosary (palpable beading at costochondral junctions), Harrison's sulcus (indentation at diaphragm attachment), pigeon chest deformity[3]
- Extremities: Widened/swollen wrists and ankles (metaphyseal widening), leg bowing (genu varum or valgum), waddling gait[3-4]
- Musculoskeletal: Proximal muscle weakness, hypotonia[1][4]
- Neurological: Chvostek sign (facial twitching on tapping facial nerve), Trousseau sign (carpal spasm with BP cuff inflation) — signs of latent tetany[9]
- Growth: Plot height/weight — assess for growth failure and stunting[3]
11. Lab Studies
- Export Lab Expected Finding in Nutritional Rickets Clinical Significance References 25-OH Vitamin D 30 nmol/L (12 ng/mL) — severe deficiency Confirms vitamin D deficiency as etiology[1-2]
- Serum calcium Low or low-normal (8.5 mg/dL) May be maintained by secondary hyperparathyroidism until late[1-2]
- Ionized calcium 4 mg/dL in symptomatic hypocalcemia More accurate than total calcium[3]
- Serum phosphate Low (4.5 mg/dL in children) Due to PTH-driven phosphaturia[2]
- Alkaline phosphatase (ALP) Elevated (>461 U/L) Reflects increased osteoblastic activity; most sensitive marker[2]
- PTH Elevated (>55 pg/mL) Secondary hyperparathyroidism[1-2]
- BUN/Creatinine Normal (unless renal cause) Rule out renal osteodystrophy[4]
- Magnesium May be low Refractory hypocalcemia if hypomagnesemia present[5]
- Urine calcium/creatinine ratio Low initially; monitor during treatment Screen for hypercalciuria with high-dose therapy[2]
12. Imaging
- First-line: AP radiographs of the wrist (distal radius/ulna) and knees — most sensitive sites for detecting rickets[4][7]
- Key findings: Metaphyseal cupping, fraying, and splaying; widened growth plates; osteopenia[3][7]
- Other findings: Rachitic rosary on chest X-ray, bowing deformities of long bones, pathologic fractures[3][7]
- Adults (osteomalacia): Looser zones (pseudofractures) — pathognomonic but only seen in severe cases; generalized osteopenia[1][24]
- Gold standard for osteomalacia: Bone biopsy with tetracycline labeling (rarely needed clinically)[1][24]
- Imaging unnecessary: Mild vitamin D insufficiency without clinical or biochemical abnormalities
13. Special Tests
- Thacher radiographic scoring system — grades severity of rickets on wrist/knee X-rays (score ≥1.5 indicates active rickets)[25]
- DEXA scan — not routinely indicated for rickets diagnosis but may assess bone mineral density in adults with osteomalacia
- Genetic testing — indicated when nutritional rickets is excluded and hereditary forms suspected (failure to respond to standard treatment, family history, consanguinity)[4][19]
- FGF23 levels — if hypophosphatemic rickets suspected (normal/low in nutritional rickets, elevated in XLH)[4][22]
14. ECG
- Indications: Obtain ECG in all patients with symptomatic hypocalcemia or serum calcium <7 mg/dL[9][21]
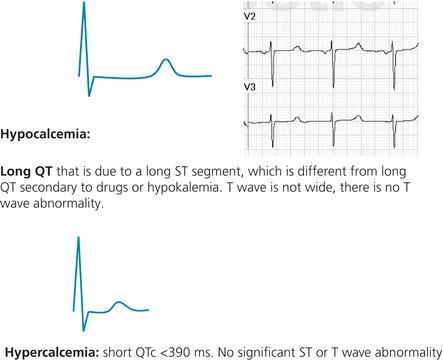
- Classic finding: Prolonged QT interval due to elongated ST segment (plateau phase of repolarization) with preserved T-wave morphology[9-10]
- Dangerous patterns: QT prolongation → torsades de pointes → ventricular fibrillation[9]
- Other: Conduction delays, signs of dilated cardiomyopathy[2]
- EKG abnormalities found in 42% of children admitted with severe vitamin D deficiency hypocalcemia in one series[21]
- The following figure illustrates the characteristic ECG changes in hypocalcemia versus hypercalcemia, highlighting the prolonged ST segment with preserved T-wave morphology that distinguishes calcium-related QT prolongation from other causes.
15. Assessment
Three stages of nutritional rickets
- Stage 1: Transient hypocalcemia → may present with seizures/tetany (especially infants)
- Stage 2: Secondary hyperparathyroidism normalizes calcium but causes hypophosphatemia → skeletal changes begin
- Stage 3: PTH can no longer maintain calcium → frank hypocalcemia + severe skeletal disease
- Severity stratification: Based on 25-OHD level, degree of hypocalcemia, presence of complications (seizures, cardiomyopathy, fractures), and radiographic severity[1][7]
- Typical presentation: Infant/toddler with bowed legs, swollen wrists, growth failure; adult with diffuse bone pain and proximal weakness[1][5]
- Complications: Hypocalcemic seizures, dilated cardiomyopathy (94% recovery with calcium correction), pathologic fractures, irreversible skeletal deformity if untreated[2][7]
16. Treatment Plan
Acute stabilization (symptomatic hypocalcemia)
- IV calcium gluconate 10%: 50–200 mg/kg/dose q6h until symptomatic improvement and serum calcium normalizes[6][15]
- Cardiac monitoring during IV calcium infusion
- Check and correct magnesium if refractory hypocalcemia[15]
- Do NOT use anticonvulsants for hypocalcemic seizures[6]
Vitamin D replacement (by age)
- Export Age Treatment Dose Duration Maintenance References 1–6 months 3,000 IU/day 8–12 weeks 400 IU/day[1-2]
- 6 months–12 years 6,000 IU/day 8–12 weeks 400–600 IU/day[1-2]
- 12–18 years 10,000 IU/day 8–12 weeks 600 IU/day[1]
- Adults 50,000 IU/week or 6,000 IU/day 8–12 weeks 1,000–2,000 IU/day[1, 3]
- Stoss therapy (poor compliance) 150,000–300,000 IU single supervised dose One-time Then maintenance[1, 4]
- Calcium supplementation: 500 mg/day elemental calcium (or 30–75 mg/kg/day in children) alongside vitamin D, especially if dietary intake is poor or hypocalcemia is present[3][18]
- Either cholecalciferol (D3) or ergocalciferol (D2) may be used; most guidelines do not prefer one over the other[14]
- Do not use calcitriol or alfacalcidol for simple nutritional rickets[15]
17. Disposition
Admit if
- Symptomatic hypocalcemia (seizures, tetany, laryngospasm)[21]
- Cardiac involvement (prolonged QT, cardiomyopathy, heart failure)[2]
- Ionized calcium <0.8 mmol/L or total calcium <7 mg/dL
- Inability to tolerate oral intake
- Observation: Moderate hypocalcemia (Ca 7–8 mg/dL) without symptoms — may observe with oral calcium and close monitoring
- Discharge if: Asymptomatic with mild biochemical abnormalities, able to take oral medications, reliable follow-up ensured
- Specialist consultation: Pediatric endocrinology (failure to respond to treatment, suspected genetic rickets), orthopedics (severe skeletal deformity), cardiology (cardiomyopathy), nephrology (renal osteodystrophy)[2][4]
18. Follow Up / Return Precautions
- Follow-up timing: Bone profile (calcium, phosphate, ALP) and 25-OHD at completion of treatment course (8–12 weeks); earlier if symptomatic[14]
- Radiographic follow-up: Wrist/knee X-rays at 3 months to assess healing (expect improvement in metaphyseal changes)[16][25]
- Lifelong maintenance supplementation recommended after treatment, at least until completion of linear growth in children[14]
- Return precautions — instruct caregivers to return immediately for:
- Seizures, muscle spasms, or twitching
- Difficulty breathing or stridor (laryngospasm)
- Poor feeding, lethargy, or irritability in infants
- New limb deformity or refusal to bear weight
- Expected recovery: Biochemical improvement within 2–4 weeks; radiographic healing by 3 months; skeletal deformities may persist if treatment is delayed[1][7]
- Prevention: All breastfed infants should receive 400 IU/day vitamin D from birth; at-risk populations require targeted supplementation[17]
References
1. Nutritional Rickets & Osteomalacia: A Practical Approach to Management. — Uday S, Högler W. The Indian Journal of Medical Research. 2020.
2. Nutritional Heart Disease And Cardiomyopathies: JACC Focus Seminar 4/4. — Sliwa K, Viljoen CA, Hasan B, Ntusi NAB. Journal of the American College of Cardiology. 2022.
3. Vitamin D, Calcium or a Combination of Vitamin D and Calcium for the Treatment of Nutritional Rickets in Children. — Chibuzor MT, Graham-Kalio D, Osaji JO, Meremikwu MM. The Cochrane Database of Systematic Reviews. 2020.
4. Rickets Guidance: Part I-Diagnostic Workup. — Haffner D, Leifheit-Nestler M, Grund A, Schnabel D. Pediatric Nephrology. 2022.
5. Vitamin D and Cardiovascular Disease: Controversy Unresolved. — Al Mheid I, Quyyumi AA. Journal of the American College of Cardiology. 2017.
6. Pearls & Oy-Sters: Focal Hypocalcemic Seizures Secondary to Severe Vitamin D Deficiency/Rickets. — Monni R, Beccaria F, Boscaini F, Frassine B, Capovilla G. Neurology. 2020.
7. Vitamin D Supplementation for Term Breastfed Infants to Prevent Vitamin D Deficiency and Improve Bone Health. — Tan ML, Abrams SA, Osborn DA. The Cochrane Database of Systematic Reviews. 2020.
8. Vitamin D and Cardiovascular Disease Will It Live Up to Its Hype?. — Lavie CJ, Lee JH, Milani RV. Journal of the American College of Cardiology. 2011.
9. American Thyroid Association Statement on Postoperative Hypoparathyroidism: Diagnosis, Prevention, and Management in Adults. — Orloff LA, Wiseman SM, Bernet VJ, et al. Thyroid : Official Journal of the American Thyroid Association. 2018.
10. Opposite Calcium Disorders, Similar Electrical Risk: Reversible Cardiomyopathy Due to Hypocalcemia and Brugada Syndrome Unmasked by Hypercalcemia. — Megid TBC, Ubida C, de Melo Sousa Ferro AC, et al. Journal of Electrocardiology. 2026.
11. Italian Association of Clinical Endocrinologists (AME) and Italian Chapter of the American Association of Clinical Endocrinologists (AACE) Position Statement: Clinical Management of Vitamin D Deficiency in Adults. — Cesareo R, Attanasio R, Caputo M, et al. Nutrients. 2018.
12. The Biological Activities of Vitamin D and Its Receptor in Relation to Calcium and Bone Homeostasis, Cancer, Immune and Cardiovascular Systems, Skin Biology, and Oral Health. — Khammissa RAG, Fourie J, Motswaledi MH, et al. BioMed Research International. 2017.
13. Enhancement of Hepatic 4-Hydroxylation of 25-Hydroxyvitamin D3 Through CYP3A4 Induction in Vitro and in Vivo: Implications for Drug-Induced Osteomalacia. — Wang Z, Lin YS, Dickmann LJ, et al. Journal of Bone and Mineral Research : The Official Journal of the American Society for Bone and Mineral Research. 2013.
14. Rickets. — Elder CJ, Bishop NJ. Lancet. 2014.
15. Rickets. — Wharton B, Bishop N. Lancet. 2003.
16. FDA Drug Label. — Updated date: 2026-01-22. Food and Drug Administration.
17. Effect of Vitamin D Supplementation on Bone Mass in Infants With 25-Hydroxyvitamin D Concentrations Less Than 50 nmol/L: A Prespecified Secondary Analysis of a Randomized Clinical Trial. — Gharibeh N, Razaghi M, Vanstone CA, et al. JAMA Pediatrics. 2023.
18. Daily versus fortnightly oral vitamin D 3 in treatment of symptomatic vitamin D deficiency in children aged 1−10 years: An open labelled randomized controlled trial. — Mondal KAP, Singh P, Singh R, Malhotra RK, Seth A. Clinical Endocrinology. 2024.
19. Rare, genetically conditioned forms of rickets: Differential diagnosis and advances in diagnostics and treatment. — Michałus I, Rusińska A. Clinical Genetics. 2018.
20. Evaluating Young Children With Fractures for Child Abuse: Clinical Report. — Haney S, Scherl S, DiMeglio L, et al. Pediatrics. 2025.
21. Characteristics of Vitamin D Deficiency Hypocalcemia Inpatient Admissions at a Single Tertiary Center. — Bustamante VH, Estrada A, Merchant N. Journal of Pediatric Endocrinology & Metabolism : JPEM. 2023.
22. X-Linked Hypophosphataemia. — Kamenický P, Briot K, Munns CF, Linglart A. Lancet. 2024.
23. Siblings with vitamin D‐dependent rickets type 1A : Importance of genetic testing and a review of genotype–phenotype correlations. — Wang LK, Shanmugasundaram M, Cooney E, Lee PDK. American Journal of Medical Genetics. Part A. 2024.
24. Spot the Silent Sufferers: A Call for Clinical Diagnostic Criteria for Solar and Nutritional Osteomalacia. — Uday S, Högler W. The Journal of Steroid Biochemistry and Molecular Biology. 2019.
25. Low Dose Depot Oral Vitamin D. Daily Oral Vitamin D for Treating Nutritional Rickets: A Randomised Clinical Trial. — Saluja RK, Dewan P, Gomber S, et al. The British Journal of Nutrition. 2021.
26. Electrocardiography. — Elias Hanna Practical Cardiovascular Medicine 2e. 2022.