Vitreous Hemorrhage
Vitreous hemorrhage (VH) is bleeding into the vitreous cavity, with an incidence of approximately 7 per 100,000 population. The most common causes are proliferative diabetic retinopathy (32–39%), r…
Vitreous hemorrhage (VH) is bleeding into the vitreous cavity, with an incidence of approximately 7 per 100,000 population. The most common causes are proliferative diabetic retinopathy (32–39%), retinal tears (12–30%), retinal vein occlusion (7–11%), and posterior vitreous detachment without retinal tear (6–8%).[1-3] The critical ED priority is ruling out retinal detachment, which occurs in up to 17% of PVD-associated VH, predominantly within the first 3 weeks.[4]
1. History
- Onset and laterality: Sudden vs. gradual; unilateral vs. bilateral
- Visual symptoms: "Shower of floaters," "cobwebs," "red/dark haze," or complete vision loss — ask about density and progression[5]
- Photopsias (flashes): Suggest vitreoretinal traction and possible retinal tear[6]
- Visual field defect: "Curtain" or "shadow" suggests retinal detachment[5]
- Timing: Onset during sleep (Valsalva-related), exertion, or spontaneous
- Trauma history: Blunt or penetrating ocular/head trauma[2]
- Prior episodes: Recurrent VH suggests proliferative retinopathy
- Diabetic history: Duration, glycemic control, prior laser/injections, last dilated exam
- Important negatives: Absence of pain (pain suggests hyphema, glaucoma, or endophthalmitis), no preceding surgery
2. Alarm Features
- Curtain-like visual field loss → retinal detachment until proven otherwise[5]
- Relative afferent pupillary defect (RAPD) → significant retinal detachment or optic nerve involvement[6]
- Elevated IOP with hyphema → secondary glaucoma requiring emergent management[7]
- "Tobacco dust" (Shafer sign) on slit lamp → vitreous pigment strongly associated with retinal tear (LR+ increases probability from 14% to 62%)[8]
- Dense VH obscuring fundus in a young male → highest risk for rhegmatogenous retinal detachment (HR 2.90 vs. women)[4]
- Bilateral VH → consider Terson syndrome (subarachnoid hemorrhage), blood dyscrasias, or leukemia
- History of trauma + VH → rule out open globe, intraocular foreign body
3. Medications
Contributors to VH
- Anticoagulants: Warfarin, rivaroxaban (ROR 11.14 for VH), dabigatran (ROR 5.83), apixaban all carry signals for intraocular hemorrhage[9]
- Antiplatelets: Aspirin, clopidogrel; combination anticoagulant + antiplatelet carries the highest risk (aOR 2.28)[10]
- Risk is dose- and adherence-dependent — higher PDC correlates with greater hemorrhage risk[10]
Treatments
- Intravitreal anti-VEGF (aflibercept, ranibizumab, bevacizumab) for PDR-related VH — regresses neovascularization while hemorrhage reabsorbs[11-12]
- Topical cycloplegics (atropine 1%) for comfort and to reduce iris movement
- Topical timolol or brimonidine if IOP elevated
- Avoid aspirin/NSAIDs acutely if not medically necessary (may worsen bleeding)
Cautions
- Do NOT routinely reverse anticoagulation unless there is concurrent acute glaucoma or open globe — shared decision-making with ophthalmology is essential[7]
- tPA (tissue plasminogen activator) intravitreal injection is experimental and not standard of care[1]
4. Diet
- No specific dietary triggers for VH
- Tight glycemic control is the most important long-term dietary/metabolic intervention for diabetic patients to reduce recurrence
- Adequate hydration; avoid excessive Valsalva maneuvers (heavy straining, constipation) which may worsen or precipitate rebleeding
- Long-term: Mediterranean-style diet and blood pressure control for patients with vascular risk factors
5. Review of Systems
- Ophthalmologic: Floaters, flashes, visual field deficits, eye pain, prior eye surgeries or injections
- Neurologic: Headache, nausea/vomiting (Terson syndrome — SAH), focal deficits
- Hematologic: Easy bruising, epistaxis, gingival bleeding (coagulopathy, blood dyscrasias)
- Endocrine: Polyuria, polydipsia, known diabetes, HbA1c history
- Cardiovascular: Hypertension, prior stroke/TIA, atrial fibrillation
- Constitutional: Fevers, weight loss (consider intraocular lymphoma, leukemia, endophthalmitis)
6. Collateral History and Family History
- Collateral: Medication list (especially anticoagulants/antiplatelets), recent procedures, compliance with diabetic eye care
- Family history: Diabetes, sickle cell disease, bleeding disorders, retinal detachment
- Social context: Occupation (monocular patients or those reliant on vision for work need expedited management), substance use (cocaine — hypertensive crisis), contact sports (trauma risk)
7. Risk Factors
- Proliferative diabetic retinopathy — most common cause; VH develops in ~46–48% of PDR eyes over 5 years even with treatment[11]
- Diabetes mellitus (poorly controlled)
- Hypertension — associated with retinal vein occlusion and macroaneurysm[2]
- Anticoagulant/antiplatelet use[9-10]
- Sickle cell disease — major cause in Black patients (>15% of spontaneous VH)[2]
- High myopia — predisposes to PVD and retinal tears[6]
- Age 45–65 — peak PVD incidence; younger patients with VH from PVD have higher RRD risk[4][6]
- Male sex — HR 2.90 for RRD in PVD-associated VH[4]
- Prior vitreoretinal surgery
- Ocular trauma
8. Differential Diagnosis
- Retinal detachment — cannot-miss; curtain-like field loss, may coexist with VH; 17% of PVD-associated VH develop RRD[4]
- Posterior vitreous detachment (without tear) — benign floaters/flashes, no hemorrhage or minimal hemorrhage
- Retinal tear without detachment — flashes, shower of floaters, vitreous pigment
- Central/branch retinal vein occlusion — painless vision loss, flame hemorrhages, cotton-wool spots
- Wet age-related macular degeneration — subretinal hemorrhage extending into vitreous[13]
- Terson syndrome — bilateral VH in setting of SAH; check for headache, altered mental status
- Intraocular tumor (melanoma, retinoblastoma, lymphoma) — mass on ultrasound[14]
- Retinal macroaneurysm — frequently overlooked, often diagnosed late; associated with hypertension[3]
- Sickle cell retinopathy — "sea fan" neovascularization[2]
- Open globe injury — trauma history, irregular pupil, low IOP
- Endophthalmitis — painful, post-procedural, hypopyon
9. Past Medical History
- Diabetes mellitus — duration, type, HbA1c, prior PRP or anti-VEGF injections
- Hypertension — control status
- Sickle cell disease/trait — hemoglobin electrophoresis if unknown
- Prior retinal tears, detachments, or vitreoretinal surgery
- Prior vitreous hemorrhage episodes
- Bleeding disorders or liver disease
- Recent intraocular procedures (injections, cataract surgery)
- History of high myopia
10. Physical Exam
- Visual acuity: Ranges from mildly decreased to light perception only depending on density; document carefully[12]
- Confrontation visual fields: Assess for field cuts suggesting retinal detachment[6]
- Pupillary exam: Check for RAPD (suggests extensive retinal detachment or optic nerve pathology)[6]
Slit lamp biomicroscopy
- Focus beam behind the lens into the anterior vitreous — have patient look up, then down, then straight ahead to mobilize blood[8]
- Look for red blood cells suspended in vitreous (confirms VH)
- "Tobacco dust" (Shafer sign) — pigmented cells = retinal tear until proven otherwise[8]
- Check anterior chamber for hyphema
- Assess for iris neovascularization (rubeosis iridis) before dilation[12]
- IOP measurement: Elevated IOP suggests ghost cell glaucoma, hemolytic glaucoma, or neovascular glaucoma[1]
- Dilated fundoscopy: If view permits, assess for retinal tears, detachment, neovascularization, vein occlusion, macroaneurysm[12]
- Indirect ophthalmoscopy with scleral depression: Even with dense VH, the peripheral retina can often be examined[6]
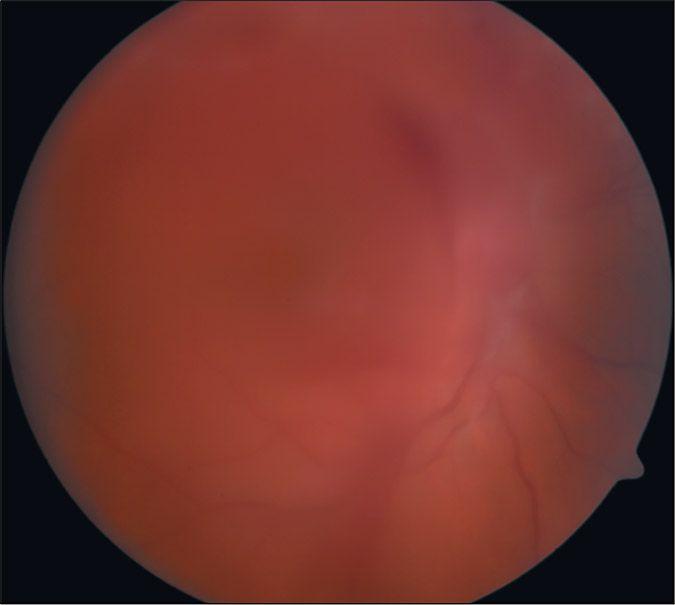
- The following figure demonstrates the fundoscopic appearance of vitreous hemorrhage with layered blood obscuring retinal details:
- View full figure Figure 3. Fundus Photograph of Vitreous Hemorrhage Acute-Onset Floaters and Flashes: Is This Patient at Risk for Retinal Detachment?. JAMA. November 24, 2009.
11. Lab Studies
- Glucose / HbA1c — screen for or assess diabetic control
- CBC with differential — anemia, thrombocytopenia, leukemia
- Coagulation studies (PT/INR, PTT) — if on anticoagulants or suspected coagulopathy
- Sickle cell screen / hemoglobin electrophoresis — in at-risk populations (Black patients, Mediterranean descent)[2]
- ESR/CRP — if giant cell arteritis or vasculitis suspected
- Blood pressure — not a lab, but critical to document; hypertension drives vein occlusion and macroaneurysm
Labs to rule out dangerous conditions
- Lipid panel, renal function — vascular risk stratification
- Blood cultures if endophthalmitis suspected
12. Imaging
First-line
- B-scan ultrasonography — mandatory when fundus view is obscured[6][14]
- Identifies retinal detachment, retinal tears (sensitivity 44–100%), mass lesions, and vitreous membranes
- Serial B-scans recommended (weekly) until VH clears or retinal status is confirmed[6]
When to image
- All dense VH obscuring the fundus
- Suspected retinal detachment
- Trauma (also CT orbits to rule out foreign body/fracture)
Gold standard
- Dilated fundoscopic exam by ophthalmology once VH clears sufficiently
Imaging NOT typically needed
- Mild VH with clear fundus view and identifiable benign cause
- CT/MRI of brain — only if Terson syndrome suspected (headache, altered mental status)
13. Special Tests
Point-of-care ultrasound (POCUS)
- Emergency physicians can use ocular POCUS to distinguish VH from retinal detachment — VH appears as echogenic material swirling within the vitreous cavity ("washing machine" sign), while retinal detachment shows a tethered, undulating membrane[15-16]
Diagnostic scoring / risk stratification
- Two-thirds of patients with VH and vitreous hemorrhage have at least one retinal break; presence of VH increases the probability of retinal tear from 14% baseline to ~62%[6][8]
- Male sex and younger age are independent risk factors for RRD in PVD-associated VH[4]
Other tests
- Fluorescein angiography — once media clears; identifies neovascularization, vein occlusion, macroaneurysm
- OCT (optical coherence tomography) — evaluates macular edema, PVD staging[6]
- Gonioscopy — if neovascular glaucoma or angle neovascularization suspected[12]
14. ECG
- Not routinely indicated for isolated VH
Obtain ECG if
- Suspected atrial fibrillation (patient on anticoagulation)
- Terson syndrome workup (SAH → cardiac arrhythmias)
- Vascular risk factor assessment in patients with retinal vein occlusion
- No specific ECG pattern is diagnostic of VH
15. Assessment
- Clinical summary: VH presents as acute, painless, monocular vision loss with floaters. Severity ranges from mild visual haze to complete loss of light perception depending on hemorrhage density. The prognosis depends entirely on the underlying etiology.[17]
Severity stratification
- Mild: Floaters, reduced acuity but fundus partially visible → likely observation
- Moderate: Significant acuity loss, fundus partially obscured → B-scan, close follow-up
- Dense: No fundus view, light perception only → urgent B-scan, ophthalmology consultation, high suspicion for retinal tear/detachment
Typical vs. atypical presentations
- Typical: Painless floaters/vision loss in a diabetic or elderly patient with PVD
- Atypical: Bilateral VH (Terson syndrome, leukemia), painful VH (hyphema + glaucoma), VH in a child (consider abuse, retinoblastoma)
- Complications: Ghost cell glaucoma, hemolytic glaucoma, hemosiderotic glaucoma, proliferative vitreoretinopathy, hemosiderosis bulbi[1]
16. Treatment Plan
Initial stabilization (ED)
- Elevate head of bed 30–45° — allows blood to settle inferiorly, clearing the visual axis[6]
- Bilateral patching may aid settling (per AAO)[6]
- Avoid anticoagulants/antiplatelets if safely possible; coordinate with prescribing physician
- Bed rest / activity restriction — avoid Valsalva, heavy lifting, bending
Medical management
- Observation — appropriate for mild-moderate VH without retinal tear/detachment; spontaneous clearance occurs at ~1% per day; 62% of PVD-associated VH clear spontaneously[1][4]
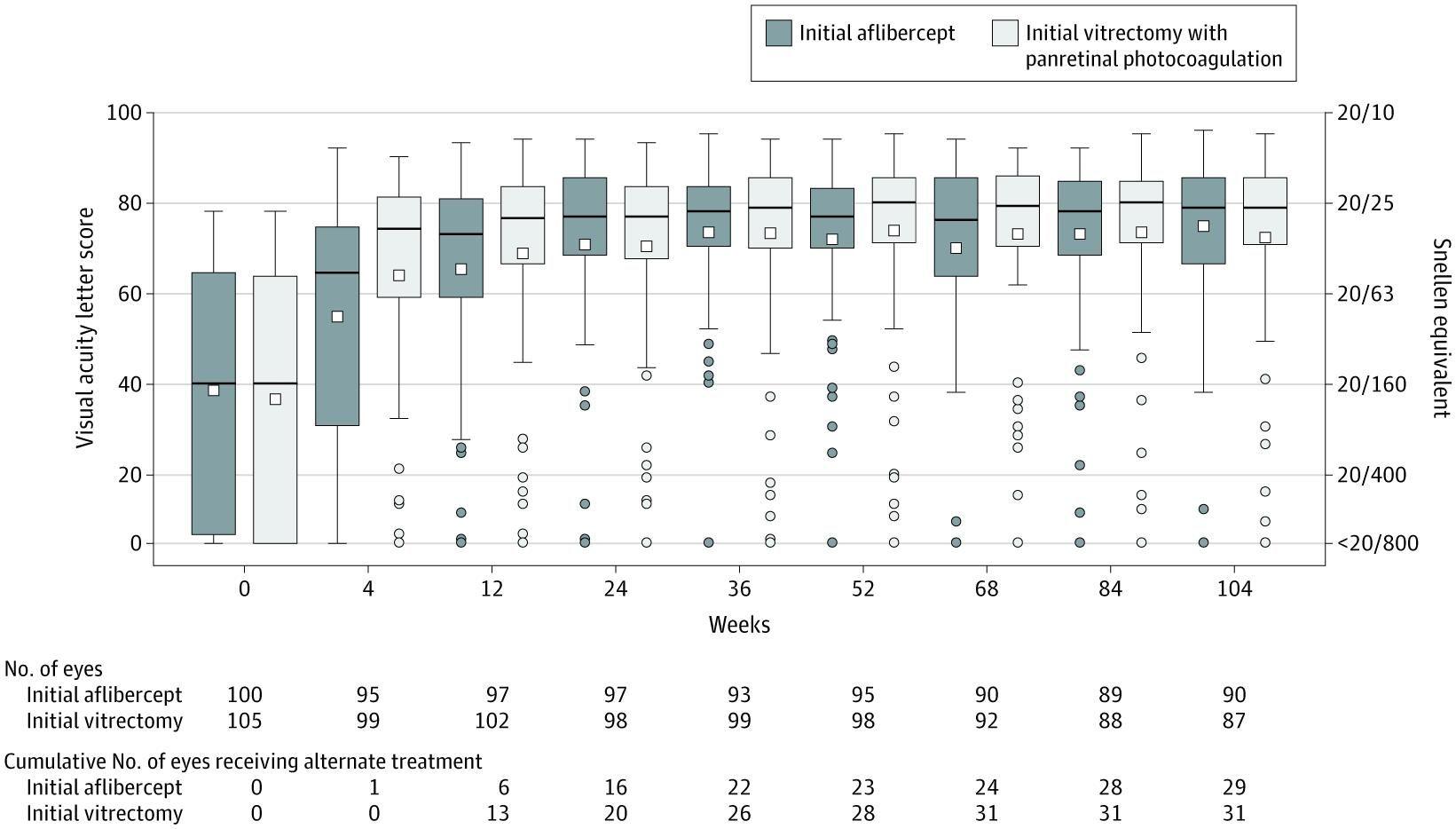
- Intravitreal anti-VEGF (aflibercept 2 mg) — for PDR-related VH; DRCR Protocol AB showed similar 2-year visual outcomes to vitrectomy, though visual recovery is slower initially[11][18]
Surgical management
- Pars plana vitrectomy (PPV) — cornerstone of treatment for nonclearing VH[12][17]
- Indications: nonclearing VH (typically observed 1–3 months), tractional retinal detachment threatening macula, combined rhegmatogenous/tractional RD, dense premacular hemorrhage[12]
- DRVS showed improved outcomes when vitrectomy is performed within 1–6 months vs. waiting 1 year[12]
- Vitrectomy provides faster initial visual recovery (significant at 4 weeks) but equivalent outcomes by 12 weeks onward[11][18]
- The following figure from the DRCR Protocol AB trial illustrates visual acuity trajectories comparing initial aflibercept vs. vitrectomy with PRP over 2 years:
- Laser photocoagulation / cryotherapy — for identified retinal tears once media clears[17]
- Preoperative anti-VEGF before vitrectomy reduces intraoperative bleeding and surgical duration[12]
17. Disposition
Emergent ophthalmology consultation (same day)
- Retinal detachment identified or strongly suspected
- Open globe / penetrating trauma
- Acute secondary glaucoma (elevated IOP with hyphema)
- Terson syndrome (concurrent SAH)
- Suspected endophthalmitis
Urgent ophthalmology referral (within 24–48 hours)
- Dense VH obscuring fundus with negative B-scan — needs serial follow-up[6]
- VH with vitreous pigment ("tobacco dust") — high probability of retinal tear[8]
- New VH in a known diabetic without recent ophthalmology evaluation
Outpatient follow-up (within 1–2 weeks)
- Mild VH with clear fundus, no retinal tear/detachment, known benign etiology (e.g., PVD in elderly)
Admission criteria
- Concurrent retinal detachment requiring emergent surgery
- Terson syndrome / SAH
- Open globe requiring surgical repair
- Acute glaucoma unresponsive to medical management
- Most patients with isolated VH can be discharged from the ED with close ophthalmology follow-up.[15]
18. Follow Up / Return Precautions
Follow-up timing
- Weekly ophthalmology visits initially for dense VH with serial B-scans until fundus is visible or retinal status confirmed[6]
- Every 1–2 weeks for moderate VH
- RRD risk is highest in the first 3 weeks — vigilant monitoring during this period is critical[4]
- Return precautions — instruct patients to return immediately for:
- New curtain or shadow in vision (retinal detachment)
- Sudden worsening of vision
- New eye pain or redness (glaucoma, rebleeding)
- New flashes of light
Patient counseling
- Keep head elevated while sleeping
- Avoid straining, heavy lifting, bending at the waist
- Avoid blood thinners if medically safe (coordinate with PCP/cardiologist)
- VH may take weeks to months to clear; after 60 days, only ~48% have cleared spontaneously[4]
- Nonclearing VH (>3 months) may require vitrectomy (median 98 days in one series)[4]
Expected recovery
- Prognosis depends on underlying cause — PDR-related VH has higher recurrence rates
- With appropriate treatment, most patients achieve significant visual improvement (mean VA improvement to ~20/40 range in surgical series)[18]
References
1. Vitreous Hemorrhage. — Spraul CW, Grossniklaus HE. Survey of Ophthalmology. 1997.
2. Spontaneous and Traumatic Vitreous Hemorrhage. — Dana MR, Werner MS, Viana MA, Shapiro MJ. Ophthalmology. 1993.
3. A Prospective Study of Dense Spontaneous Vitreous Hemorrhage. — Lindgren G, Sjödell L, Lindblom B. American Journal of Ophthalmology. 1995.
4. Vitreous Hemorrhage Due to Posterior Vitreous Detachment: Incidence of Retinal Detachment and Spontaneous Clearance During Observation. — Hasbolat H, Christensen UC, Lund-Andersen C. Ophthalmology. 2026.
5. Sudden Vision Loss: A Diagnostic Approach. — Fraser JA, Son M, Vinokurtseva A. American Family Physician. 2025.
6. Posterior Vitreous Detachment, Retinal Breaks, and Lattice Degeneration Preferred Practice Pattern®. — Kim SJ, Bailey ST, Kovach JL, et al. Ophthalmology. 2025.
7. Spontaneous Hyphema and Vitreous Hemorrhage Causing Secondary Glaucoma in a Patient on Apixaban. — Stenberg RT, Nelson J, Rabinowitz J, Simon EL. The Journal of Emergency Medicine. 2023.
8. Acute-Onset Floaters and Flashes: Is This Patient at Risk for Retinal Detachment?. — Hollands H, Johnson D, Brox AC, et al. The Journal of the American Medical Association. 2009.
9. Risk of Intraocular Hemorrhage With New Oral Anticoagulants. — Talany G, Guo M, Etminan M. Eye. 2017.
10. Antithrombotic Medications and Intraocular Hemorrhage Risk in Exudative Age-Related Macular Degeneration. — Kim MS, Nam S, Lee J, Woo SJ. JAMA Network Open. 2025.
11. Effect of Intravitreous Aflibercept vs Vitrectomy With Panretinal Photocoagulation on Visual Acuity in Patients With Vitreous Hemorrhage From Proliferative Diabetic Retinopathy: A Randomized Clinical Trial. — Antoszyk AN, Glassman AR, Beaulieu WT, et al. The Journal of the American Medical Association. 2020.
12. Diabetic Retinopathy Preferred Practice Pattern®. — Lim JI, Kim SJ, Bailey ST, et al. Ophthalmology. 2025.
13. Epidemiology of the Association Between Anticoagulants and Intraocular Hemorrhage in Patients With Neovascular Age-Related Macular Degeneration. — Kiernan DF, Hariprasad SM, Rusu IM, et al. Retina. 2010.
14. Causes of Vitreous Hemorrhage. — Lindgren G, Lindblom B. Current Opinion in Ophthalmology. 1996.
15. Point-of-Care Ultrasonography in the Diagnosis of Retinal Detachment, Vitreous Hemorrhage, and Vitreous Detachment in the Emergency Department. — Lahham S, Shniter I, Thompson M, et al. JAMA Network Open. 2019.
16. Point-of-Care Ultrasound for the Evaluation of Non-Traumatic Visual Disturbances in the Emergency Department: The VIGMO Protocol. — Gandhi K, Shyy W, Knight S, Teismann N. The American Journal of Emergency Medicine. 2019.
17. Vitreous Hemorrhage - Causes, Diagnosis, and Management. — Shaikh N, Srishti R, Khanum A, et al. Indian Journal of Ophthalmology. 2023.
18. Visual Acuity, Vitreous Hemorrhage, and Other Ocular Outcomes After Vitrectomy vs Aflibercept for Vitreous Hemorrhage Due to Diabetic Retinopathy: A Secondary Analysis of a Randomized Clinical Trial. — Glassman AR, Beaulieu WT, Maguire MG, et al. JAMA Ophthalmology. 2021.