Von Willebrand Disease (Bleeding)
Von Willebrand disease (VWD) is the most common inherited bleeding disorder, caused by quantitative or qualitative defects in von Willebrand factor (VWF), a glycoprotein essential for platelet adhe…
Von Willebrand disease (VWD) is the most common inherited bleeding disorder, caused by quantitative or qualitative defects in von Willebrand factor (VWF), a glycoprotein essential for platelet adhesion and factor VIII stabilization.[1-2] Prevalence of the VWD trait is ~1%, with symptomatic disease affecting ~0.1% of the population.[3] The following is a clinically structured summary for emergency and primary care management.
1. History
- Bleeding pattern: Predominantly mucocutaneous — epistaxis, easy bruising, gingival bleeding, bleeding from minor wounds, menorrhagia[1-2]
- Timing: Lifelong history; symptoms often begin in childhood with bruising and nosebleeds[2]
- Triggers: Surgical/dental procedures, trauma, menses, childbirth — 60–80% of patients bleed after surgery or dental extractions[2][4]
- Severity: Ranges from mild (type 1) to life-threatening (type 3); ask about transfusion history, iron deficiency, hospitalizations for bleeding[3]
- Progression: Bleeding may worsen with age in type 2/3 (GI angiodysplasia); may improve with age in some type 1 patients due to rising VWF with aging[1]
- Important negatives: Absence of deep tissue/joint bleeding argues against severe VWD or hemophilia; absence of petechiae argues against thrombocytopenia
2. Alarm Features
- GI bleeding from angiodysplasia — most common life-threatening complication, especially in elderly patients with type 2 or 3 VWD[2]
- CNS/intracranial hemorrhage — rare (0–8% prevalence) but catastrophic[3]
- Postpartum hemorrhage — reported in 6–59% of affected women[3]
- Hemarthrosis — suggests severe disease (type 3 or type 2N) with very low FVIII levels[2]
- Hemodynamic instability, rapidly expanding hematoma, or uncontrolled surgical bleeding — requires emergent VWF/FVIII concentrate replacement[5]
3. Medications
- Desmopressin (DDAVP): First-line for type 1 VWD minor bleeding; raises VWF/FVIII 2–4 fold for 8–12 hours. Administer IV, SC, or intranasal. Confirm response with a prior desmopressin challenge[6-8]
- Contraindicated/ineffective: Type 3 (no stored VWF), type 2B (can worsen thrombocytopenia), generally poor response in types 2A, 2M, 2N GeneReviews® [Internet]. Updated 2024 Nov 14.[9-10]
- Caution: Hyponatremia (10% incidence in children despite fluid restriction); tachyphylaxis with repeated dosing; limit fluid intake[6][11]
- VWF replacement concentrates: Mainstay for moderate/severe bleeding, type 2 and 3 VWD, and major surgery. Options include plasma-derived VWF/FVIII products (e.g., Humate-P) and recombinant VWF (Vonvendi, approved ≥18 years) GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- For type 2N and type 3, prefer products containing both VWF and FVIII GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Antifibrinolytics: Tranexamic acid (oral, IV, or topical) — effective as stand-alone for minor mucosal bleeding or as adjunct[6][9]
- Relatively contraindicated with gross hematuria (risk of ureteral clot obstruction) GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Hormonal therapy: Combined oral contraceptives or levonorgestrel IUD for heavy menstrual bleeding — recommended over desmopressin per ASH/ISTH/NHF/WFH guidelines[6]
- Agents to AVOID: Aspirin, clopidogrel, fish oil, turmeric supplements; NSAIDs should be used cautiously and only briefly GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
4. Diet
- Avoid supplements that impair hemostasis: Fish oil, vitamin E in high doses, turmeric/curcumin, ginkgo biloba GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Iron-rich diet: Critical for patients with chronic blood loss (menorrhagia, GI bleeding) to prevent/treat iron deficiency anemia[6]
- Hydration: Fluid restriction required after desmopressin administration to prevent hyponatremia[6]
5. Review of Systems
- Hematologic: Bruising frequency/size, epistaxis duration, gum bleeding, prolonged bleeding from cuts
- GYN: Menstrual duration, pad/tampon count, clot passage, postpartum hemorrhage history
- GI: Melena, hematochezia, hematemesis (angiodysplasia screening)
- MSK: Joint swelling, pain, limited range of motion (hemarthrosis in severe disease)
- Neuro: Headache, altered mental status (intracranial hemorrhage)
- Hematuria, post-procedural bleeding history
6. Collateral History and Family History
- Autosomal dominant inheritance in most types (types 1, 2A, 2B, 2M); autosomal recessive in types 2N and 3[1]
- Ask about family members with known bleeding disorders, excessive surgical/dental bleeding, menorrhagia, or transfusion history
- Patients often carry a medical alert bracelet and may travel with their own factor replacement and treatment plan from a hemophilia treatment center[5]
- Blood group O is associated with ~25% lower VWF levels, which can confound diagnosis[1]
7. Risk Factors
- Family history of VWD or bleeding disorder
- Blood group O (lower baseline VWF levels)[1]
- Female sex — menorrhagia and postpartum hemorrhage increase clinical detection[2]
- Hypothyroidism — can lower VWF levels[1]
- Medications — antiplatelet agents, NSAIDs, anticoagulants exacerbate bleeding risk GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
8. Differential Diagnosis
- Hemophilia A — low FVIII but normal VWF; X-linked; deep tissue/joint bleeding predominates. Type 2N VWD mimics hemophilia A (impaired VWF-FVIII binding)[10]
- Platelet function disorders (e.g., Glanzmann thrombasthenia, Bernard-Soulier syndrome) — mucocutaneous bleeding pattern similar to VWD; distinguished by platelet aggregation studies[12]
- Acquired von Willebrand syndrome — associated with lymphoproliferative disorders, aortic stenosis, hypothyroidism, autoimmune disease; new-onset bleeding in older adults without family history[1]
- Thrombocytopenia (ITP, TTP, DIC) — check platelet count
- Liver disease/coagulopathy — check PT/INR, hepatic function
- Child abuse — consider in pediatric patients with unexplained bruising (VWD workup helps exclude)
9. Past Medical History
- Prior bleeding episodes and their management (desmopressin response, factor replacement use)
- Previous surgeries and hemostatic complications
- History of iron deficiency anemia or transfusions
- Known VWD subtype and baseline VWF/FVIII levels
- Hepatitis B/C status (relevant if exposed to blood products prior to 1985) GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Chronic conditions: hypothyroidism, liver disease, renal disease
10. Physical Exam
- Vital signs: Tachycardia, hypotension (hemorrhagic shock in severe bleeding)
- Skin: Ecchymoses (often large, disproportionate to trauma), petechiae (less common than in platelet disorders)
- HEENT: Active epistaxis, gingival oozing, oropharyngeal bleeding
- Abdomen: Tenderness, distension (GI hemorrhage, retroperitoneal bleed)
- MSK: Joint effusions, limited ROM (hemarthrosis — suggests severe disease)[2]
- GU: Menorrhagia assessment, hematuria
- Neuro: Mental status changes, focal deficits (intracranial hemorrhage)
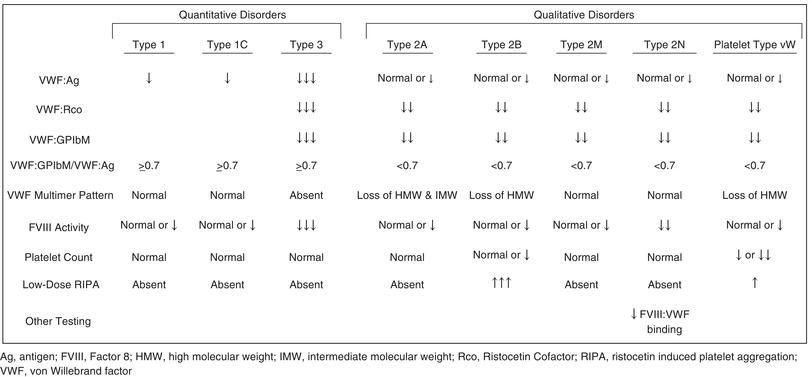
11. Lab Studies
- The following figure summarizes expected laboratory values by VWD subtype:
First-line panel
- VWF antigen (VWF:Ag) — quantifies VWF protein
- VWF activity (VWF:RCo, VWF:GPIbR, or VWF:GPIbM) — measures platelet-binding function
- Factor VIII activity — often reduced, especially in types 2N and 3
- CBC with platelet count — thrombocytopenia may occur in type 2B
- Screening tests: PT (usually normal), aPTT (may be prolonged if FVIII is low)
- Diagnostic thresholds: VWF levels ≤30 IU/dL = definite VWD; 30–50 IU/dL = possible VWD/"low VWF"[15]
Subtyping tests (second-line)
- VWF:Activity/VWF:Ag ratio ≤0.6 → suggests type 2
- VWF multimer analysis
- Low-dose ristocetin-induced platelet aggregation (RIPA) — enhanced in type 2B
- VWF:FVIII binding assay — abnormal in type 2N
- VWF propeptide — helps distinguish type 1 from type 3
- Adjunct labs: Iron studies, ferritin (chronic blood loss), type and screen, blood group
12. Imaging
- Not routinely indicated for diagnosis of VWD itself
- CT head without contrast — if concern for intracranial hemorrhage
- CT abdomen/pelvis — for suspected retroperitoneal or intra-abdominal hemorrhage
- Upper/lower endoscopy — for GI bleeding; evaluate for angiodysplasia (especially in elderly type 2/3 patients)[2][9]
- Joint ultrasound or MRI — for suspected hemarthrosis or arthropathy assessment GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
13. Special Tests
- ISTH Bleeding Assessment Tool (BAT): Standardized scoring system for bleeding severity; useful for screening but limited by cumulative scoring and age dependence[2]
- Desmopressin challenge test: Administer DDAVP and measure VWF/FVIII at 1 and 4 hours; a "responder" shows ≥2-fold increase with levels >50 IU/dL sustained at 4 hours[6][8]
- Platelet function analyzer (PFA-100/200): Prolonged closure time suggests VWD but is not specific; normal result does not exclude VWD
- Light transmission aggregometry (LTA): Helps distinguish VWD from platelet function disorders[12]
- Genetic testing: Informative for severe type 1, type 2, and type 3 VWD; not useful for most mild type 1 or "low VWF"[14]
14. ECG
- Not directly indicated for VWD diagnosis
- Obtain if hemodynamically significant bleeding with tachycardia, hypotension, or suspected myocardial ischemia from anemia
- Consider in patients with acquired von Willebrand syndrome associated with aortic stenosis (murmur on exam)
15. Assessment
- Type 1 (60–80% of cases): Partial quantitative deficiency; mild-moderate mucocutaneous bleeding; generally good desmopressin response[1][3]
- Type 2 (~20% of cases): Qualitative defects; variable severity; subtypes (2A, 2B, 2M, 2N) have distinct management implications[1]
- Type 3 (<5% of cases): Near-complete absence of VWF; severe bleeding including hemarthrosis and life-threatening hemorrhage; risk of VWF alloantibody (inhibitor) development[2][9]
- Complications to anticipate: Iron deficiency anemia, arthropathy (severe disease), GI angiodysplasia bleeding, postpartum hemorrhage, procedure-related hemorrhage[2-3]
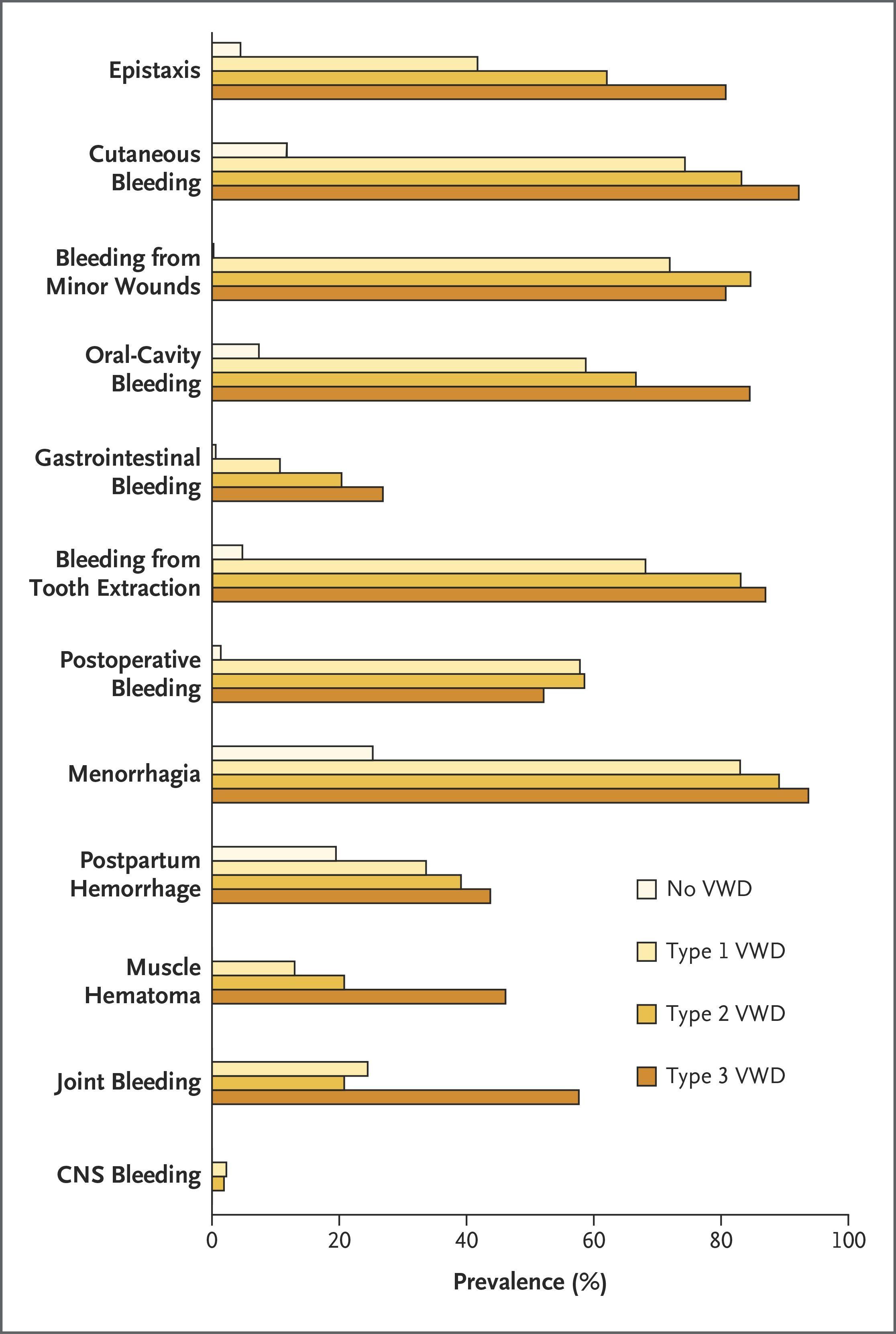
- The following figure illustrates the frequency of bleeding symptoms across VWD subtypes compared to controls:
- View full figure Figure 3. Frequency of Bleeding Symptoms in Adults with von Willebrand’s Disease. Von Willebrand’s Disease. N Engl J Med. November 23, 2016.
16. Treatment Plan
Acute Bleeding — Emergency Management
Minor mucosal bleeding (epistaxis, oral, menstrual)
- Tranexamic acid 1g IV/PO q6–8h (or topical) ± desmopressin (if known type 1 responder)[6][9]
- Local measures: nasal packing, direct pressure
- Moderate bleeding (prolonged epistaxis, dental extraction, minor surgery):
- Desmopressin 0.3 mcg/kg IV/SC (type 1 responders)[6][8]
- OR VWF/FVIII concentrate if desmopressin-unresponsive or type 2/3[5][9]
- Adjunctive tranexamic acid
- Severe/life-threatening bleeding (GI hemorrhage, intracranial, major trauma, postpartum):
- VWF/FVIII concentrate (e.g., Humate-P) — target VWF:RCo and FVIII >80–100%[5]
- Cryoprecipitate or FFP only if concentrates unavailable (multiple units needed)[5]
- Tranexamic acid as adjunct (avoid if hematuria) GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- RBC transfusion for significant anemia; platelet transfusion if type 2B with severe thrombocytopenia GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Use patient's own factor products if available — per National Bleeding Disorders Foundation recommendation[5]
Long-Term / Outpatient Management
- Antifibrinolytics (tranexamic acid) for recurrent mucosal bleeding[6][11]
- Hormonal therapy for heavy menstrual bleeding[6]
- Long-term VWF prophylaxis for severe/recurrent bleeding (type 3, severe type 2)[4]
- Iron supplementation for chronic blood loss[6]
- Comprehensive care at a hemophilia treatment center GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
17. Disposition
Admit if
- Hemodynamically significant bleeding or active hemorrhage requiring factor replacement
- GI bleeding, suspected intracranial hemorrhage, or postpartum hemorrhage
- Need for serial VWF/FVIII monitoring and repeated dosing
- Severe anemia requiring transfusion
Observe if
- Moderate bleeding controlled with desmopressin/antifibrinolytics but requiring monitoring for rebleeding
- Post-desmopressin monitoring for hyponatremia (especially pediatric patients)[6]
Discharge if
- Minor mucosal bleeding controlled with local measures and/or oral tranexamic acid
- Known mild type 1 VWD with established outpatient treatment plan
- Hemodynamically stable with no ongoing active bleeding
- Consult hematology for: any patient with unknown VWD subtype presenting with significant bleeding, type 2B or type 3 disease, need for factor replacement, or perioperative planning GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
18. Follow Up / Return Precautions
- Follow-up: Hematology within 1–2 weeks after ED visit for bleeding; annual comprehensive assessment at a bleeding disorders center including CBC, iron studies, VWF levels, and treatment efficacy review GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Return immediately for: Recurrent or worsening bleeding, signs of GI hemorrhage (melena, hematemesis), severe headache or neurologic changes, lightheadedness/syncope, heavy menstrual bleeding soaking >1 pad/hour
Patient counseling
- Wear medical alert identification[5]
- Avoid aspirin, NSAIDs (use acetaminophen for pain), and supplements that impair hemostasis GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Avoid high-contact sports; use protective equipment GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- No invasive procedures (including dental work, piercings, circumcision) without prior hematology consultation GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Carry treatment plan and factor products when traveling[5]
- Ensure hepatitis B vaccination GeneReviews® [Internet]. Updated 2024 Nov 14.[9]
- Expected course: Most patients with type 1 VWD have a good prognosis with appropriate on-demand treatment; type 2 and 3 patients may require lifelong prophylaxis and have higher morbidity from recurrent bleeding and arthropathy[2][4]
References
1. Von Willebrand Disease. — Seidizadeh O, Eikenboom JCJ, Denis CV, et al. Nature Reviews. Disease Primers. 2024.
2. Von Willebrand’s Disease. — Leebeek FW, Eikenboom JC. The New England Journal of Medicine. 2016.
3. Clinical, economic, and health‐related quality of life burden associated with von Willebrand disease in adults and children: Systematic and targeted literature reviews. — Castaman G, Katsarou O, Jansen N, et al. Haemophilia : The Official Journal of the World Federation of Hemophilia. 2023.
4. Effectiveness of long‐term prophylaxis using pdFVIII / VWF concentrate in patients with inherited von Willebrand disease. — Rugeri L, Harroche A, Repessé Y, et al. European Journal of Haematology. 2022.
5. Hematologic Emergencies: Recognition and Initial Management. — Jones DE, Walker JJ, Abellada AMP. American Family Physician. 2024.
6. Low von Willebrand Factor in Children and Adolescents: A Review. — Srivaths L, Kouides PA. JAMA Pediatrics. 2021.
7. How I Treat Von Willebrand Disease. — Castaman G. Thrombosis Research. 2020.
8. Desmopressin as a hemostatic and blood sparing agent in bleeding disorders. — Mohinani A, Patel S, Tan V, et al. European Journal of Haematology. 2023.
9. Von Willebrand Disease. — Johnsen J GeneReviews® [Internet]. 2024.
10. How I Treat Type 2 Variant Forms of Von Willebrand Disease. — Tosetto A, Castaman G. Blood. 2015.
11. Use of the von Willebrand factor concentrate with low factor VIII content to manage patients with inherited von Willebrand disease requiring surgical or secondary long‐term prophylaxis: An expert opinion paper from an Italian panel. — Castaman G, Borchiellini A, Coppola A, et al. European Journal of Haematology. 2022.
12. Rare bleeding disorders: Advances in management. — Haemophilia : The Official Journal of the World Federation of Hemophilia. 2024.
13. Coagulation concentrates for inherited bleeding disorders. — Gary M. Woods, Robert F. Sidonio Rossi's Principles of Transfusion Medicine 6e. 2022.
14. New Advances in the Diagnosis of Von Willebrand Disease. — Sharma R, Haberichter SL. Hematology. American Society of Hematology. Education Program. 2019.
15. Diagnosis and Management of Von Willebrand Disease: Guidelines for Primary Care. — Yawn B, Nichols WL, Rick ME. American Family Physician. 2009.