Warfarin-induced Skin Necrosis
Warfarin-induced skin necrosis is a rare (<0.1% prevalence) but devastating complication of warfarin therapy caused by occlusive microthrombi in dermal and subcutaneous venules and capillaries, typ…
Warfarin-induced skin necrosis is a rare (<0.1% prevalence) but devastating complication of warfarin therapy caused by occlusive microthrombi in dermal and subcutaneous venules and capillaries, typically presenting 3–8 days after warfarin initiation.[1-3] It results from a transient hypercoagulable state due to the rapid decline of protein C (short half-life ~6 hours) before the reduction of procoagulant factors II, IX, and X.[2][4] If not rapidly recognized and treated, it can be fatal.[1]
1. History
- Timing is the critical clue: Onset typically 3–8 days after warfarin initiation; can occur as early as day 1 in the setting of HIT[2][4-5]
- Ask about recent warfarin start or dose increase, especially use of a loading dose[6-7]
- Characterize skin lesions: initial pain and paresthesia in affected area → erythematous plaques → hemorrhagic bullae → black necrotic eschar[1][8]
- Location: preferentially affects fat-rich areas — breasts, buttocks, hips, thighs, abdomen[1][9]
- Ask about prior episodes of WISN — previously uncomplicated warfarin courses do not preclude future episodes[10]
- Inquire about known thrombophilia history (protein C, protein S, antithrombin III deficiency, Factor V Leiden)[1-2][9]
- Ask about pregnancy/postpartum status — reduced free protein S levels increase risk[10]
2. Alarm Features
- Rapidly expanding painful erythema with hemorrhagic bullae in a patient recently started on warfarin
- Full-thickness skin necrosis progressing to gangrene — may require amputation of limbs, breast, or penis[3]
- Concurrent HIT (heparin-induced thrombocytopenia) dramatically increases risk of venous limb gangrene[9][11]
- Supratherapeutic INR in the setting of new skin lesions[11]
- Systemic signs: sepsis from secondary wound infection, DIC
- Acral necrosis (fingers, toes) — suggests venous limb gangrene, a distinct and more severe entity often associated with HIT[9]
3. Medications
- Causative agent: Warfarin (and other vitamin K antagonists/coumarins)[2][6]
- Higher loading doses significantly increase risk — avoid loading doses, especially in patients with known protein C/S deficiency[7][12]
Treatment medications
- Vitamin K (phytonadione) IV to reverse warfarin effect[1]
- Unfractionated heparin (UFH) for continued anticoagulation[1][4]
- Protein C concentrate (human) — has shown benefit in halting necrosis progression[1][5]
- Fresh frozen plasma (FFP) — provides protein C and other factors, though less effective than protein C concentrate[5]
- Prevention: In patients with known protein C/S deficiency, initiate warfarin at low dose (≤5 mg) with concurrent heparin for 5–7 days[3][12]
- Contraindication: Do NOT restart warfarin in patients who have had WISN without careful risk-benefit analysis; consider DOACs as alternatives
4. Diet
- Not directly applicable to the acute condition
- Patients on warfarin should maintain consistent vitamin K intake to avoid INR fluctuations[3]
- Adequate protein and caloric intake is important for wound healing in necrotic tissue management
5. Review of Systems
- Skin: New painful areas, color changes, blistering, areas of numbness
- Extremities: Swelling, discoloration of fingers/toes (purple toe syndrome is a separate entity)
- Hematologic: Easy bruising, bleeding from other sites (gums, urine, stool)
- Neurologic: Paresthesias in affected areas
- Constitutional: Fever (suggests secondary infection of necrotic tissue)
- GU: Penile involvement can occur — ask about genital pain/swelling in males[3]
6. Collateral History and Family History
- Family history of thrombophilia: Protein C deficiency, protein S deficiency, antithrombin III deficiency, Factor V Leiden[1-2]
- Family history of neonatal purpura fulminans — associated with homozygous protein C deficiency[2]
- Prior VTE events in patient or family members
- Confirm exact warfarin dose, start date, and whether a loading dose was used[7]
- Confirm whether heparin bridging was used at initiation[4]
- Social context: Obtain accurate medication list including herbals/supplements that may affect INR[3]
7. Risk Factors
- Protein C deficiency (hereditary or acquired) — highest risk, even heterozygotes[1-2]
- Protein S deficiency[2][10]
- Antithrombin III deficiency[1]
- Factor V Leiden[9]
- Large loading doses of warfarin[6-7]
- Female sex[1]
- Obesity[1]
- Postpartum state (physiologically reduced free protein S)[10]
- Concurrent HIT — dramatically increases risk of venous limb gangrene[9][11]
- Initiation of warfarin without heparin bridging in at-risk patients[3-4]
- Active malignancy with consumptive coagulopathy[9]
8. Differential Diagnosis
- Necrotizing fasciitis — deeper tissue involvement, systemic toxicity, crepitus; requires surgical exploration[6][13]
- Heparin-induced skin necrosis — different mechanism (platelet aggregation); can occur at injection sites and distally[1]
- Warfarin-associated calciphylaxis — occurs much later (average 32 months), favors lower extremities, associated with chronic vascular calcification rather than acute protein C depletion[14]
- Purpura fulminans (DIC-related) — widespread, not limited to fat-bearing areas
- Cholesterol crystal embolization / atheroemboli — "blue toe syndrome," livedo reticularis[3]
- Venous limb gangrene — acral distribution, often in setting of HIT + warfarin[9]
- Decubitus ulcers — pressure-dependent distribution, no hemorrhagic bullae[13]
- Cellulitis/abscess — warmth, fluctuance, no hemorrhagic bullae
- Pyoderma gangrenosum — undermined violaceous borders, pathergy
9. Past Medical History
- Prior episodes of VTE (DVT, PE) — the indication for warfarin
- Known thrombophilia or hypercoagulable state
- Previous warfarin use — prior uncomplicated courses do NOT exclude future WISN[10]
- HIT history — critical to identify[3][9]
- Malignancy — consumptive coagulopathy increases risk[9]
- Liver disease — affects baseline coagulation factor synthesis
- Renal disease — consider calciphylaxis as alternative diagnosis[14]
10. Physical Exam
- Vital signs: Fever (secondary infection), tachycardia (pain, sepsis)
Skin
- Early: Painful, well-demarcated erythematous plaques in fat-bearing areas[1]
- Intermediate: Petechiae → ecchymoses → hemorrhagic bullae with surrounding retiform purpura[8][14]
- Late: Full-thickness black necrotic eschar[1][8]
- Distribution: Breasts, buttocks, hips, thighs, abdomen — areas with abundant subcutaneous fat[1][9]
- Acral exam: Check fingers, toes, penis for involvement — acral necrosis suggests venous limb gangrene rather than classic WISN[9]
- Wound assessment: Depth of necrosis, signs of secondary infection (purulence, crepitus, expanding erythema)
- Peripheral pulses: Typically preserved (microvascular thrombosis, not macrovascular)[9]
11. Lab Studies
- INR/PT — often supratherapeutic; however, WISN can occur at therapeutic INR[11]
- Protein C activity level — typically markedly depressed; draw BEFORE administering FFP or protein C concentrate
- Protein S activity level (free and total)
- Antithrombin III level
- CBC with platelet count — rule out concurrent HIT (platelet drop >50%)[5]
- HIT antibody (PF4/heparin ELISA) and serotonin release assay if HIT suspected[11]
- D-dimer, fibrinogen — assess for DIC
- Blood cultures — if secondary infection suspected
- Factor V Leiden and prothrombin gene mutation — for thrombophilia workup (can be deferred to outpatient)
12. Imaging
- Imaging is generally NOT required for diagnosis — WISN is a clinical and histopathologic diagnosis
- Doppler ultrasound of extremities if concurrent DVT suspected (especially in HIT setting)
- CT/MRI may be considered to assess depth of tissue necrosis if surgical planning is needed
- Plain radiographs — may show subcutaneous calcification if calciphylaxis is in the differential[14]
13. Special Tests
Skin biopsy — gold standard for confirmation
- Histopathology shows diffuse dermal microthrombi with endothelial cell damage, red cell extravasation, and progression to full-thickness coagulative necrosis[8]
- Distinguishes from necrotizing fasciitis, calciphylaxis, and other mimics[8]
- 4T Score for HIT probability if concurrent HIT is suspected
- Thrombophilia panel (protein C, protein S, antithrombin III, Factor V Leiden, prothrombin G20210A) — ideally drawn before treatment but can be deferred; warfarin itself lowers protein C/S levels, complicating interpretation
14. ECG
- ECG is not directly diagnostic for WISN
- Obtain if the patient has atrial fibrillation (common indication for warfarin) or if hemodynamically unstable
- Rule out PE (sinus tachycardia, right heart strain pattern) if concurrent thromboembolic disease is suspected
15. Assessment
- Warfarin-induced skin necrosis is a dermatologic emergency driven by microvascular thrombosis from a transient hypercoagulable state during warfarin initiation. Key clinical pearls:
- Prevalence: ~1 in 10,000 warfarin-treated patients, representing ~2% of those with protein C deficiency[1]
- The classic presentation — painful erythematous plaques in fat-bearing areas 3–8 days after warfarin initiation — is highly characteristic[1-2][4]
- Atypical presentations include acral involvement (consider venous limb gangrene + HIT) and late-onset lesions (consider warfarin-associated calciphylaxis)[9][14]
- Severity ranges from localized skin necrosis to extensive full-thickness involvement requiring amputation[3]
- Mortality is significant if not promptly recognized and treated[1]
16. Treatment Plan
Immediate management
- Stop warfarin immediately[3]
- Administer IV vitamin K (phytonadione) to reverse warfarin effect[1]
- Start therapeutic heparin (UFH or LMWH) for continued anticoagulation — ensure HIT has been excluded before using heparin[1][4]
- Protein C concentrate (human) — if available, administer to replete protein C levels; has demonstrated arrest of necrosis progression within 24 hours[5]
- FFP — alternative source of protein C if concentrate unavailable[5]
Wound management
- Surgical consultation for debridement of necrotic tissue[1][3]
- Skin grafting may be required for extensive wounds[1][5]
- Wound care with appropriate dressings; monitor for secondary infection
Long-term anticoagulation
- Transition to a DOAC (direct oral anticoagulant) if continued anticoagulation is needed — DOACs do not carry the same risk of skin necrosis
- If warfarin must be reused (rare), initiate at ≤5 mg/day with concurrent heparin for at least 5–7 days, ensuring therapeutic INR on two consecutive days before stopping heparin[3-4][12]
17. Disposition
- Admit all patients with suspected or confirmed WISN — this is a dermatologic emergency requiring:
- IV anticoagulation
- Possible protein C replacement
- Surgical wound assessment
- Monitoring for progression
- ICU admission if extensive necrosis, hemodynamic instability, sepsis, or concurrent HIT with limb-threatening gangrene
- Consult: Hematology (thrombophilia workup, protein C replacement), Dermatology (biopsy, wound management), Surgery/Plastics (debridement, grafting)
- Discharge only after necrosis has stabilized, alternative anticoagulation is established, and wound care plan is in place
18. Follow Up / Return Precautions
- Follow-up with hematology within 1–2 weeks for thrombophilia workup results and long-term anticoagulation planning
- Wound care follow-up with surgery/plastics as needed for graft monitoring
- Return precautions: Return immediately for new skin lesions, expanding necrosis, fever, wound drainage, or signs of bleeding
Patient counseling
- WISN is documented as a warfarin allergy/adverse reaction in the medical record
- Inform all future providers of this history
- If protein C/S deficiency is confirmed, genetic counseling and family screening should be considered
- Expected course: With prompt treatment, necrosis progression halts within 24–48 hours; wound healing may take weeks to months depending on extent; skin grafting may be required[5]
- Relevant images 2 items
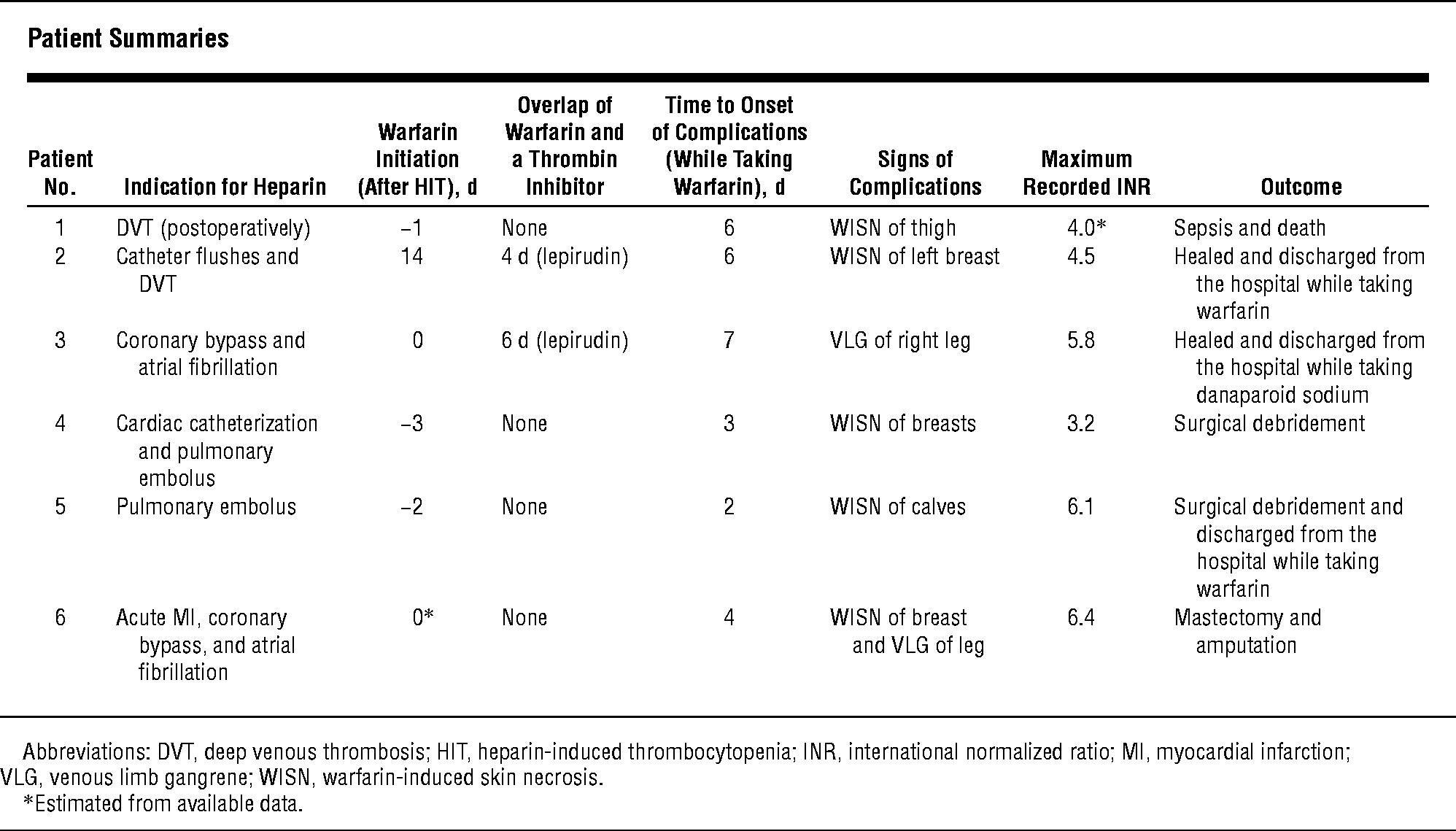
- Table 1
- Arch Intern Med January 11, 2004
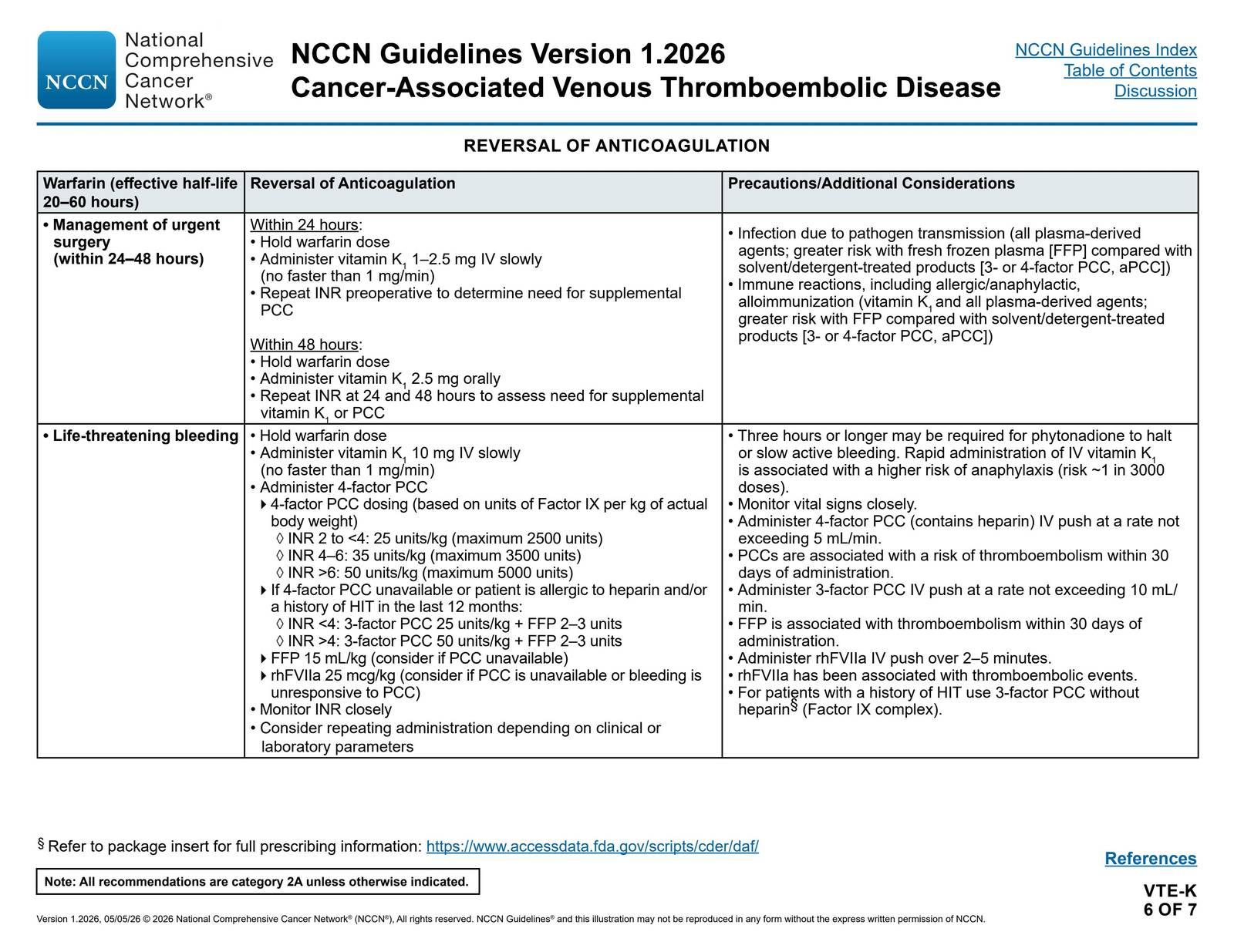
- Cancer-Associated Venous Thromboembolic Disease: Reversal of Anticoagulation — NCCN Guidelines® — Cancer-Associated Venous Thromboembolic Disease p. 45 (v1.2026)
- NCCN May 4, 2026
References
1. Severe Adverse Cutaneous Reactions to Drugs. — Roujeau JC, Stern RS. The New England Journal of Medicine. 1994.
2. Oral Anticoagulant Drugs. — Hirsh J. The New England Journal of Medicine. 1991.
3. FDA Drug Label. — Updated date: 2025-06-17. Food and Drug Administration.
4. Management of Venous Thromboembolism. — Ginsberg JS. The New England Journal of Medicine. 1996.
5. Warfarin-Induced Skin Necrosis Treated With Protein C Concentrate (Human). — Stewart A. American Journal of Health-System Pharmacy : AJHP : Official Journal of the American Society of Health-System Pharmacists. 2010.
6. Warfarin Induced Skin Necrosis. — Chan YC, Valenti D, Mansfield AO, Stansby G. The British Journal of Surgery. 2000.
7. Warfarin Skin Necrosis. The Role of Factor VII. — Jones RR, Cunningham J. The British Journal of Dermatology. 1979.
8. Warfarin-Induced Skin Necrosis. — Nazarian RM, Van Cott EM, Zembowicz A, Duncan LM. Journal of the American Academy of Dermatology. 2009.
9. Ischemic Limb Gangrene with Pulses. — Warkentin TE. The New England Journal of Medicine. 2015.
10. Warfarin Skin Necrosis in a Postpartum Woman With Protein S Deficiency. — Cheng A, Scheinfeld NS, McDowell B, Dokras AA. Obstetrics and Gynecology. 1997.
11. Warfarin-Induced Skin Necrosis and Venous Limb Gangrene in the Setting of Heparin-Induced Thrombocytopenia. — Srinivasan AF, Rice L, Bartholomew JR, et al. Archives of Internal Medicine. 2004.
12. Care of Patients Receiving Long-Term Anticoagulant Therapy. — Schulman S. The New England Journal of Medicine. 2003.
13. Warfarin-Induced Necrosis of the Skin. — DeFranzo AJ, Marasco P, Argenta LC. Annals of Plastic Surgery. 1995.
14. Warfarin-Associated Nonuremic Calciphylaxis. — Yu WY, Bhutani T, Kornik R, et al. JAMA Dermatology. 2017.
15. Cancer-Associated Venous Thromboembolic Disease. — Updated 2026-05-05. National Comprehensive Cancer Network.