Wernicke's Encephalopathy
Wernicke's encephalopathy (WE) is an acute, life-threatening but reversible neurological emergency caused by thiamine (vitamin B1) deficiency. The classic triad of mental status changes, oculomotor…
Wernicke's encephalopathy (WE) is an acute, life-threatening but reversible neurological emergency caused by thiamine (vitamin B1) deficiency. The classic triad of mental status changes, oculomotor dysfunction, and gait ataxia is present in fewer than one-third of cases, making a high index of suspicion essential.[1-2] If untreated, approximately 80% of survivors progress to irreversible Korsakoff syndrome (chronic amnesia with confabulation), and mortality reaches ~20%.[2-3]
1. History
- Duration and pattern of alcohol use (quantity, frequency, last drink)
- Recent weight loss, poor oral intake, prolonged vomiting, or diarrhea
- Onset and progression of confusion, visual changes, unsteadiness
- History of bariatric surgery, hyperemesis gravidarum, chemotherapy, prolonged TPN, or restrictive eating
- Recent hospitalization with glucose-containing IV fluids without thiamine supplementation
- Prior episodes of similar symptoms or known Korsakoff syndrome[4-5]
- Thiamine stores deplete within 2 weeks of deficient intake; symptoms can appear as early as 1 week[6]
2. Alarm Features
- Coma or progressive obtundation — indicates severe thalamic/brainstem involvement[7]
- Hypothermia — posterior hypothalamic involvement[2][8]
- Hypotension and tachycardia — cardiovascular beriberi or autonomic dysfunction[2][7]
- Seizures — glutamatergic hyperactivity from thiamine deficiency[8]
- Optic disc edema or retinal hemorrhages — can be presenting features[7]
- Progression to Korsakoff syndrome — anterograde/retrograde amnesia with confabulation signals irreversible damage[2][4]
- Concurrent sepsis or lactic acidosis may be prodromal signs of severe thiamine deficiency[5]
3. Medications
- Thiamine IV is the cornerstone treatment (see Treatment Plan below)
- Administer thiamine BEFORE glucose — carbohydrate metabolism consumes thiamine as a cofactor and can precipitate or worsen WE[9]
- Magnesium must be repleted — patients with hypomagnesemia may fail to respond to thiamine[5][10]
- Loop diuretics (furosemide) increase urinary thiamine losses and worsen deficiency[11-12]
- Proton pump inhibitors combined with diuretics may exacerbate hypomagnesemia, impairing thiamine response[5]
- Metformin and chronic alcohol use can contribute to lactic acidosis in the setting of thiamine deficiency
- Thiamine has an excellent safety profile; anaphylaxis from IV thiamine is exceedingly rare[2]
4. Diet
- Acute: NPO or limited intake is common in these patients; parenteral thiamine is essential since oral absorption is unreliable in malnourished/alcoholic patients[7]
- Refeeding syndrome risk: WE symptoms commonly arise during refeeding; monitor electrolytes closely (phosphorus, magnesium, potassium)[5][10]
- Long-term: Balanced diet with thiamine-rich foods (whole grains, legumes, pork, fortified cereals)
- Polished rice diets, excessive refined carbohydrates, and "junk food" diets increase relative thiamine requirements[13]
- Chronic alcohol impairs thiamine absorption in the jejunum and inhibits conversion to active forms[10]
5. Review of Systems
- Neuro: Confusion, memory loss, diplopia, blurred vision, unsteadiness, numbness/tingling in extremities, hearing loss
- Cardiac: Dyspnea, orthopnea, peripheral edema, palpitations (wet beriberi)[6-7]
- GI: Nausea, vomiting, abdominal pain, anorexia, diarrhea, weight loss[5][7]
- Autonomic: Urinary retention, dizziness, tachycardia[5]
- Psych: Apathy, hallucinations, behavioral disturbances, confabulation[7]
6. Collateral History and Family History
- Collateral from family/friends is critical: duration and severity of alcohol use, recent dietary intake, functional decline, prior episodes of confusion
- Assess for social isolation, homelessness, food insecurity
- Family history of alcohol use disorder
- Genetic susceptibility: variants in thiamine transporter genes (SLC19A2, SLC19A3) may predispose to deficiency at lower thresholds[7]
- History of prior WE episodes or known Korsakoff syndrome
7. Risk Factors
- Alcohol use disorder — most common cause in the US/Western countries[2][10]
- Malnutrition/malabsorption: bariatric surgery, hyperemesis gravidarum, anorexia nervosa, prolonged vomiting, chronic diarrhea[1][5]
- Malignancy — especially GI cancers, chemotherapy-induced vomiting[14-15]
- Prolonged TPN without thiamine supplementation[11]
- Chronic illness: HIV/AIDS, end-stage liver disease, renal dialysis[4][16]
- Refeeding after prolonged starvation[5]
- Loop diuretic use — increases urinary thiamine excretion[11]
- Hospitalized patients receiving IV dextrose without thiamine[9][17]
8. Differential Diagnosis
- Export Diagnosis Distinguishing Features References Hepatic encephalopathy Asterixis, elevated ammonia, liver disease stigmata; may coexist with WE[1-2]
- Alcohol withdrawal / delirium tremens Tremor, autonomic hyperactivity, seizures; timeline after cessation; may coexist[3-4]
- Stroke (bilateral thalamic) Acute onset, vascular risk factors, DWI restricted diffusion in vascular territory[5]
- Autoimmune/viral encephalitis CSF pleocytosis, antibodies (NMDAR, LGI1), fever[6]
- Metronidazole-induced encephalopathy Similar MRI pattern; medication history[5]
- Marchiafava-Bignami disease Corpus callosum lesions, alcohol-related[5, 7]
- Central pontine myelinolysis History of rapid sodium correction, pontine lesions[5]
- Meningitis Fever, meningismus, CSF abnormalities[5]
- Toxic ingestion Methanol, ethylene glycol — osmolar gap, metabolic acidosis[5]
9. Past Medical History
- Prior episodes of WE or known Korsakoff syndrome
- Alcohol use disorder — duration, severity, prior withdrawal episodes
- GI surgery (especially bariatric procedures, gastrectomy, fundoplication)
- Chronic liver disease, pancreatitis
- Malignancy, chemotherapy history
- Eating disorders (anorexia nervosa, bulimia)
- HIV/AIDS
- Dialysis
10. Physical Exam
- Vitals: Hypothermia, hypotension, tachycardia — all raise suspicion[2][8]
- Mental status: Confusion, apathy, disorientation, inability to concentrate, confabulation; may range to stupor or coma[7]
- Eyes: Horizontal nystagmus (most common ocular finding), bilateral lateral rectus palsy (CN VI), conjugate gaze palsy, sluggish pupillary response, anisocoria, papilledema[7-8]
- Gait: Wide-based ataxia, inability to tandem walk, may be unable to stand; ranges from mild unsteadiness to complete inability to ambulate[7]
- Peripheral neuro: Diminished deep tendon reflexes, distal sensory loss (coexistent polyneuropathy)[3][6]
- Cardiac: Signs of high-output heart failure (bounding pulses, peripheral edema, JVD) in wet beriberi[6-7]
- Nutritional status: Cachexia, temporal wasting, glossitis, angular cheilitis
11. Lab Studies
- Serum thiamine (vitamin B1) level — draw BEFORE supplementation; however, results are often delayed and should NOT delay treatment[1][20]
- Erythrocyte transketolase activity — more specific but not widely available[8]
- Serum magnesium — must be corrected for thiamine to be effective[5][10]
- Comprehensive metabolic panel — electrolytes, glucose, renal/hepatic function
- Serum lactate — may be elevated due to impaired pyruvate metabolism[5][10]
- Phosphorus — refeeding syndrome risk; supplement if <1 mg/dL[10]
- CBC, lipase, ammonia, coagulation studies — assess for concurrent hepatic disease, pancreatitis
- Blood alcohol level
- Other nutritional labs: folate, B12, B6
12. Imaging
- MRI brain (with and without contrast) is the imaging modality of choice
- Sensitivity ~53%, specificity ~93%[7]
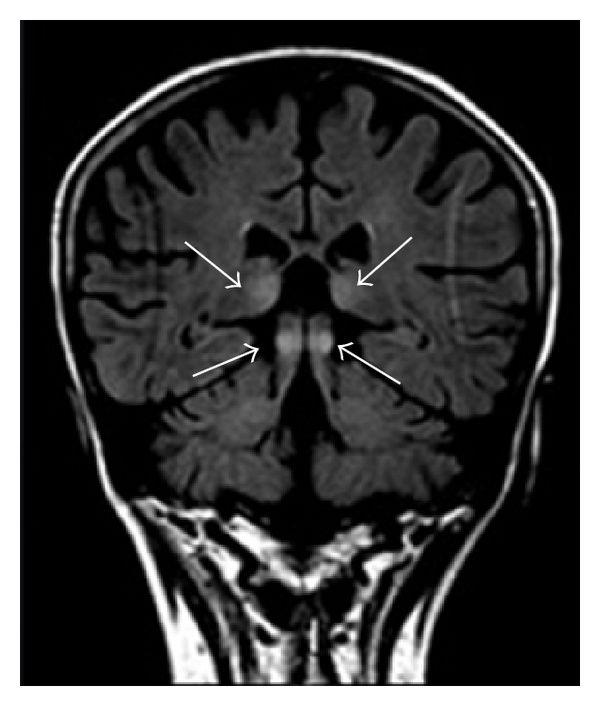
- Typical findings: symmetric T2/FLAIR hyperintensities in medial thalami, mammillary bodies, periaqueductal gray, tectal plate, floor of the fourth ventricle[1][8]
- DWI may show restricted diffusion (reversible cytotoxic edema)[20-21]
- Contrast enhancement, especially of mammillary bodies[22]
- Atypical sites: corpus callosum splenium, fornix, cerebral cortex, cerebellar vermis[20]
- The following figure demonstrates the characteristic bilateral symmetric thalamic hyperintensities seen on MRI in acute WE:
- View full figure Figure 5. (a)Read more MR Imaging Findings in Alcoholic and Nonalcoholic Acute Wernicke’s Encephalopathy: A Review. Biomed Res Int. January 14, 2014.
- CT head — usually negative in acute WE; may show hypodensities in bilateral thalami in some cases[8][22]
- Imaging is supportive but NOT required to initiate treatment — WE is a clinical diagnosis and treatment should not be delayed for imaging[2]
13. Special Tests
- Caine Criteria (operational diagnostic criteria for WE) — requires ≥2 of 4:[7-8]
- Dietary deficiency / malnutrition
- Oculomotor abnormalities
- Cerebellar dysfunction
- Altered mental state or mild memory impairment
- More sensitive than the classic triad, especially in alcoholic patients[7][15]
- Therapeutic test: Clinical improvement after parenteral thiamine administration supports the diagnosis[7][23]
- Point-of-care glucose — check before and during treatment
- EEG: Normal early; nonspecific diffuse slowing (theta range) in later stages[7]
14. ECG
- ECG findings relate primarily to wet beriberi (cardiovascular thiamine deficiency):
- Sinus tachycardia — most common finding[6][13]
- T-wave abnormalities (nonspecific ST-T changes)[13]
- Low voltage in severe cases
- Signs of right heart strain in high-output failure
- ECG is indicated in all patients with suspected WE to evaluate for concurrent cardiovascular beriberi[6-7]
- Arrhythmias may occur in the setting of concurrent electrolyte derangements (hypomagnesemia, hypokalemia)
15. Assessment
- WE is a clinical diagnosis — the classic triad is present in only ~10–33% of cases[1-2]
- Maintain a low threshold for empiric treatment given the excellent safety profile of thiamine and the devastating consequences of missed diagnosis[2][15]
- Autopsy studies show WE prevalence of 0.4–2.8%, with the majority undiagnosed antemortem[1]
- Atypical presentations are common in non-alcoholic patients, who often present with isolated altered mental status[8]
Severity stratification
- Mild: Nystagmus + confusion in a malnourished patient
- Moderate: Full triad present
- Severe: Coma, hypothermia, cardiovascular collapse, extensive brainstem involvement on MRI — associated with poor prognosis and high mortality[18]
16. Treatment Plan
Initial Stabilization
- ABCs, IV access, continuous monitoring
- Administer thiamine BEFORE or concurrent with glucose[9-10]
Thiamine Replacement — Dosing varies by guideline
- Export Guideline / Source Acute Dosing Maintenance References Royal College of Physicians 500 mg IV TID × 2–3 days 250 mg IV/IM daily × 3–5 days, then oral[1-2]
- EFNS 200 mg IV TID Transition to oral[2]
- ASAM (prophylaxis in alcohol withdrawal) 100 mg IV/IM daily × 3–5 days Oral thiamine[3]
- FDA label 100 mg IV initially, then 50–100 mg IM daily Until balanced diet[4]
- JAMA Review (2026) 100–200 mg IV TID × 3 days 100 mg PO daily long-term[5]
- High-dose IV thiamine (500 mg TID) is increasingly favored for confirmed or strongly suspected WE, as 100 mg doses may be insufficient to restore vitamin status or prevent progression[7][24]
- Dilute in 100 mL NS, infuse over 30 minutes[7]
- Correct hypomagnesemia — essential for thiamine to function[5][10]
- Correct other electrolyte abnormalities (phosphorus, potassium)[10]
- Multivitamin supplementation including folate and B12
Expected Response to Treatment
- Ocular abnormalities improve within hours to days[6]
- Confusion improves over days to weeks[25]
- Gait ataxia improves gradually and often incompletely[6]
- Amnesia may be permanent if Korsakoff syndrome has developed[2-3]
17. Disposition
- Admit all patients with suspected or confirmed WE — this is a medical emergency[1][26]
- ICU admission for: coma, hemodynamic instability, hypothermia, respiratory failure, concurrent severe alcohol withdrawal[10][18]
- Observation/step-down for patients with mild presentations responding to thiamine
- Neurology consultation for atypical presentations, diagnostic uncertainty, or failure to improve
- Psychiatry/addiction medicine consultation for concurrent alcohol use disorder[4]
- Nutrition/dietetics consultation for refeeding management
18. Follow Up / Return Precautions
- Outpatient follow-up within 1–2 weeks after discharge
- Continue oral thiamine 100 mg daily long-term for high-risk individuals[9]
- Neuropsychological testing if persistent cognitive deficits to evaluate for Korsakoff syndrome
- Alcohol use disorder treatment — referral to addiction medicine, counseling, pharmacotherapy (naltrexone, acamprosate)
- Return precautions: new or worsening confusion, visual changes, inability to walk, falls, seizures, chest pain, shortness of breath
- Expected recovery: Ocular findings resolve most completely; gait ataxia improves partially; memory deficits may be permanent[6]
- Patient/family counseling: Emphasize the critical importance of continued thiamine supplementation, adequate nutrition, and alcohol cessation to prevent recurrence
References
1. Wernicke Encephalopathy: A Mini Review of the Clinical Spectrum, Atypical Manifestations, and Diagnostic Challenges. — Li S, Xing C. Frontiers in Neurology. 2025.
2. Wernicke Encephalopathy-Clinical Pearls. — Sinha S, Kataria A, Kolla BP, Thusius N, Loukianova LL. Mayo Clinic Proceedings. 2019.
3. Thiamine for Prevention and Treatment of Wernicke-Korsakoff Syndrome in People Who Abuse Alcohol. — Day E, Bentham PW, Callaghan R, Kuruvilla T, George S. The Cochrane Database of Systematic Reviews. 2013.
4. A Case for Early High-Dose Thiamine—Moving From Reaction to Prevention. — Goldstein DN, Hunter AJ, Riquelme PA. JAMA Internal Medicine. 2025.
5. A Clinician's View of Wernicke-Korsakoff Syndrome. — Wijnia JW. Journal of Clinical Medicine. 2022.
6. Nutritional neuropathies. — Gwathmey KG, Grogan J. Muscle & Nerve. 2020.
7. Wernicke's Encephalopathy: New Clinical Settings and Recent Advances in Diagnosis and Management. — Sechi G, Serra A. The Lancet. Neurology. 2007.
8. MR Imaging Findings in Alcoholic and Nonalcoholic Acute Wernicke’s Encephalopathy: A Review. — Manzo G, De Gennaro A, Cozzolino A, et al. BioMed Research International. 2014.
9. Peripheral Neuropathy. — Mauermann ML, Staff NP. The Journal of the American Medical Association. 2026.
10. Clinical Practice Guideline on Alcohol Withdrawal Management. — Anika Alvanzo MD MS DFASAM FACP, Kurt Kleinschmidt MD FASAM, Julie A. Kmiec DO FASAM, et al American Society of Addiction Medicine (2020). 2020.
11. Cardiomyopathy in Children: Classification and Diagnosis: A Scientific Statement From the American Heart Association. — Lipshultz SE, Law YM, Asante-Korang A, et al. Circulation. 2019.
12. Current Aspects of Thiamine Deficiency on Heart Function. — Roman-Campos D, Cruz JS. Life Sciences. 2014.
13. Reappearance of Beriberi Heart Disease in Japan. A Study of 23 Cases. — Kawai C, Wakabayashi A, Matsumura T, Yui Y. The American Journal of Medicine. 1980.
14. Case Report: Wernicke's Encephalopathy Induced by Prolonged Fasting Due to Apparent Psychogenic Dysphagia. — Mills L, Zou H, Alnounou A, et al. Frontiers in Behavioral Neuroscience. 2026.
15. Wernicke-Korsakoff Syndrome in Patients With Cancer: A Systematic Review. — Isenberg-Grzeda E, Rahane S, DeRosa AP, Ellis J, Nicolson SE. The Lancet. Oncology. 2016.
16. Cognitive Impairment Severity in Relation to Signs of Subclinical Wernicke's Encephalopathy in HIV and Alcoholism Comorbidity. — Le Berre AP, Fama R, Sassoon SA, et al. AIDS. 2020.
17. FDA Drug Label. — Updated date: 2025-02-27. Food and Drug Administration.
18. Wernicke-Korsakoff Syndrome With Extensive Brainstem Involvement. — Li H, Ding Q, Wang K, et al. Neurology. 2025.
19. Neuroimaging in alcohol use disorder: From mouse to man. — Fritz M, Klawonn AM, Zahr NM. Journal of Neuroscience Research. 2022.
20. Typical and Atypical MRI Abnormalities in Wernicke's Encephalopathy: Correlation With Blood Vitamin B1 Levels. — Hiraga A, Kojima K, Kuwabara S. Journal of the Neurological Sciences. 2024.
21. Diffusion-Weighted Imaging Abnormalities in Wernicke Encephalopathy: Reversible Cytotoxic Edema?. — Chu K, Kang DW, Kim HJ, Lee YS, Park SH. Archives of Neurology. 2002.
22. Clinical Reasoning: A 71-Year-Old Man Receiving Treatment for Cryptococcal Meningitis, Developing New-Onset Lethargy. — Peng TJ, Kimbrough T, Tolchin BD. Neurology. 2019.
23. An Overview of Beriberi. — Pereira AG, Cunha LNP, Paiva SAR, et al. Medical Principles and Practice : International Journal of the Kuwait University, Health Science Centre. 2025.
24. Wernicke's Encephalopathy Treated With High Dose Intravenous Thiamine: A case Report. — Alamir M, Cantu-Weinstein A, Branning R, Weleff J, Anand A. Journal of Addictive Diseases. 2025.
25. Teaching NeuroImages: Wernicke Encephalopathy: Diagnostically Deceptive but Treatable. — Cerejo R, Newey C, Stillman M. Neurology. 2013.
26. Wernicke Encephalopathy in a Patient With Medullary Infarctions: A Case Report. — Wang L, Song GJ, Su HJ. The Journal of International Medical Research. 2024.