West Nile Virus Encephalitis
West Nile virus (WNV) encephalitis is a neuroinvasive disease caused by a neurotropic flavivirus transmitted primarily by Culex species mosquitoes. It is the leading cause of mosquito-borne encepha…
West Nile virus (WNV) encephalitis is a neuroinvasive disease caused by a neurotropic flavivirus transmitted primarily by Culex species mosquitoes. It is the leading cause of mosquito-borne encephalitis in the United States, with approximately 1,300 neuroinvasive cases and 129 deaths reported annually.[1] Approximately 80% of WNV infections are asymptomatic, ~20% cause a self-limited febrile illness, and <1% progress to neuroinvasive disease (meningitis, encephalitis, or acute flaccid myelitis).[1-2] Mortality of neuroinvasive disease is ~10% overall, rising to 20% in those ≥70 years and 30–40% in immunocompromised patients.[1]
1. History
- Timing/seasonality: Abrupt onset, typically July through September (peak mosquito season); incubation 2–14 days after mosquito bite[1][3]
- Prodrome: Fever, headache, fatigue, myalgia, nausea/vomiting often precede neurologic symptoms by days[4]
- Neurologic symptoms: Confusion, disorientation, stupor, personality change, lethargy lasting >24 hours; tremor (especially upper extremity, postural); myoclonus; ataxia[1][3]
- Key exposures: Recent outdoor/mosquito exposure, geographic location with known WNV activity, recent blood transfusion, organ transplantation[1]
- Immunocompromised hosts: Longer incubation (median 13.5–15 days for transfusion/transplant-acquired); may present with more subtle symptoms (myoclonus, confusion rather than headache/pain)[1][5]
- Important negatives: Absence of sensory deficits (distinguishes acute flaccid myelitis from GBS); no vesicular rash (distinguishes from HSV/VZV)[1][3]
2. Alarm Features
- Rapidly progressive altered mental status → stupor, coma[1][3]
- Acute flaccid paralysis — asymmetric limb weakness progressing over 24–48 hours, areflexic[1][3]
- Dysarthria and dysphagia — may herald diaphragmatic/intercostal paralysis and respiratory failure requiring emergent intubation[1][3]
- Seizures (3–6% of WNV encephalitis)[1]
- Signs of elevated intracranial pressure[1]
- Cardiac involvement — chest pain, new arrhythmia, or hemodynamic instability suggesting myocarditis (rare but associated with worse outcomes)[2][6]
- Autonomic instability[1]
3. Medications
- No approved antiviral therapy exists — management is entirely supportive[1]
- Corticosteroids should be used with caution: A retrospective cohort study found corticosteroid use within the first 48 hours was associated with significantly increased hospital mortality (aHR 3.93, 95% CI 1.14–13.51)[7]
- Empiric acyclovir should be started at presentation for all undifferentiated encephalitis until HSV is excluded[8-9]
- Investigational therapies (IVIG, high-titer WNV IVIG, IFN-α2b, ribavirin, monoclonal antibodies) have shown no proven benefit in controlled studies[1][9-10]
- In transplant recipients, reduction or discontinuation of immunosuppression is a key adjunctive measure[10]
- Seizure management: Standard antiepileptic drugs (levetiracetam, benzodiazepines) as needed; avoid medications that lower seizure threshold
4. Diet
- Hydration is critical — patients with encephalitis may have impaired oral intake due to altered mental status, nausea/vomiting, or dysphagia[3]
- NPO precautions if airway protective reflexes are compromised or intubation is anticipated
- Aspiration precautions — formal swallow evaluation before oral feeding in patients with bulbar dysfunction (dysarthria, dysphagia)[1]
- No specific dietary triggers or long-term dietary modifications are relevant to WNV
5. Review of Systems
- Neurologic: Headache severity, confusion, personality change, tremor, weakness (symmetric vs. asymmetric), visual changes, difficulty swallowing/speaking, gait instability[1][3]
- Constitutional: Fever pattern, fatigue, myalgia, arthralgia, weight loss[1][4]
- GI: Nausea, vomiting, diarrhea (common in WNV meningitis)[1]
- Dermatologic: Maculopapular rash (less common in neuroinvasive disease than WNV fever)[3]
- Ophthalmologic: Blurred vision, eye pain (chorioretinitis, uveitis, optic neuritis)[1-2]
- Cardiac: Chest pain, palpitations, dyspnea (rare myocarditis)[2][6]
- Urologic: Urinary retention (may occur with myelitis)
6. Collateral History and Family History
- Collateral: Baseline cognitive function, timeline of behavioral/personality changes, witnessed seizures, recent travel to endemic areas, outdoor activities (dusk-to-dawn exposure), occupational exposures (agricultural workers, outdoor laborers)
- Transplant/transfusion history: Recent organ transplantation or blood product receipt[1]
- Immunosuppression status: Medications (B-cell–depleting agents, chemotherapy, chronic corticosteroids), HIV status, hematologic malignancies[1]
- Family history: No hereditary predisposition, though genetic susceptibility (e.g., CCR5 polymorphisms) has been described[11]
7. Risk Factors
- Age ≥50 years — strongest risk factor for neuroinvasive disease; incidence and case-fatality increase markedly with advancing age[1-2]
- Immunosuppression: Solid organ transplant recipients, hematologic malignancies, B-cell–depleting monoclonal antibodies (mortality 30–40%)[1]
Comorbidities associated with increased mortality
- Chronic kidney disease (OR 5.99)
- Hypertension (OR 4.01)
- Diabetes mellitus (OR 2.43)
- Other: Cerebrovascular disease, alcohol abuse[2]
- Exposure: Living in or traveling to areas with active WNV transmission; outdoor activity during peak mosquito hours (dusk to dawn)[1]
8. Differential Diagnosis
The differential for arboviral CNS disease is broad
- Herpes simplex encephalitis (HSV-1) — temporal lobe predilection on MRI, hemorrhagic CSF; must empirically treat with acyclovir until excluded
- Other arboviral encephalitides — Eastern equine encephalitis, St. Louis encephalitis, Powassan virus, La Crosse encephalitis (geographic/seasonal overlap)
- Enteroviral meningoencephalitis — especially in pediatric patients
- Bacterial meningitis — higher CSF WBC with neutrophil predominance, low glucose, positive Gram stain/culture
- Tuberculous meningitis — subacute course, basilar meningeal enhancement, low CSF glucose
- Autoimmune encephalitis (anti-NMDAR) — psychiatric symptoms, movement disorders, younger patients; antibody testing[8]
- Metabolic/toxic encephalopathy — hepatic, uremic, drug-induced
- CNS lymphoma or carcinomatous meningitis — in immunocompromised patients
- Distinguishing features of WNV encephalitis: Extrapyramidal signs (tremor, parkinsonism, myoclonus), acute flaccid paralysis, summer/fall seasonality, deep gray matter/brainstem MRI pattern[1][3][12]
9. Past Medical History
- Prior WNV infection (IgG positivity without IgM suggests past infection, not acute)[1]
- History of organ transplantation or blood transfusion
- Immunosuppressive conditions or medications
- Chronic kidney disease, diabetes, hypertension (prognostic significance)[4]
- Prior neurologic conditions (baseline for comparison)
- Vaccination history (no human WNV vaccine exists; flavivirus vaccines such as yellow fever or Japanese encephalitis may cause serologic cross-reactivity)[1]
10. Physical Exam
- Vital signs: Fever (88% of neuroinvasive cases), tachycardia; monitor for hypertension/hypotension suggesting autonomic instability[4]
Neurologic exam (critical)
- Mental status: GCS assessment; confusion, stupor, coma[3]
- Tremor: Coarse, postural, predominantly upper extremities — highly characteristic[3]
- Myoclonus: Upper extremities and facial muscles; may persist during sleep[3]
- Cerebellar signs: Ataxia, dysmetria[3]
- Parkinsonian features: Rigidity, bradykinesia[3]
- Cranial nerves: Facial weakness (often bilateral), dysarthria, dysphagia[1][3]
- Motor: Asymmetric flaccid weakness, areflexia/hyporeflexia (acute flaccid myelitis); preserved sensation[3]
- Meningeal signs: Nuchal rigidity, Kernig/Brudzinski signs[3]
- Skin: Maculopapular rash (trunk/extremities, less common in neuroinvasive disease)[1]
- Fundoscopic exam: Chorioretinitis, vitritis, optic disc edema[1]
11. Lab Studies
CSF analysis (essential)
- Pleocytosis: Mean ~226 WBC/mm³ (range 1–7,950); lymphocytic predominance (neutrophils may predominate early)
- Protein: Elevated (mean 101 mg/dL in encephalitis, 76 mg/dL in meningitis)
- Glucose: Normal (helps distinguish from bacterial/TB meningitis)
- WNV-specific IgM in serum and CSF — primary diagnostic test; IgM in CSF confirms CNS infection (does not cross intact blood-brain barrier)[1][13]
- If initial IgM negative, repeat on or after day 8 (>98% sensitivity by day 8)[1]
- WNV RT-PCR — more sensitive in immunocompromised patients (63% CSF PCR positivity in immunosuppressed vs. 15% in immunocompetent)[1][5]
- Confirmatory PRNT (plaque reduction neutralization test) — for cross-reactive flavivirus exposure, atypical presentations, or suspected transplant-related transmission[1]
- Peripheral blood: WBC usually normal or mildly elevated; check CMP (hyponatremia, renal function), troponin if cardiac involvement suspected[3][14]
- Rule-out labs: Blood cultures, HSV PCR, enterovirus PCR, HIV, autoimmune encephalitis panel as clinically indicated[8]
12. Imaging
Brain MRI (preferred)
- May be normal in up to 30–37% of cases
- Classic findings: T2/FLAIR hyperintensities in brainstem, thalami, basal ganglia, mesial temporal structures, cerebellum
- Diffusion restriction in up to 50% of cases
- Bilateral thalamic involvement should raise strong suspicion for WNV (shared with Japanese encephalitis serocomplex)[12]
- Worse outcomes associated with signal abnormalities, meningeal involvement, and intraspinal abnormalities vs. normal MRI[1]
- Spinal MRI (if acute flaccid myelitis suspected): T2/FLAIR hyperintensity and enhancement in anterior horns, conus medullaris, cauda equina[1]
- CT head: Often normal; useful primarily to rule out mass lesion or hemorrhage before lumbar puncture
- Chest imaging: If respiratory compromise suspected
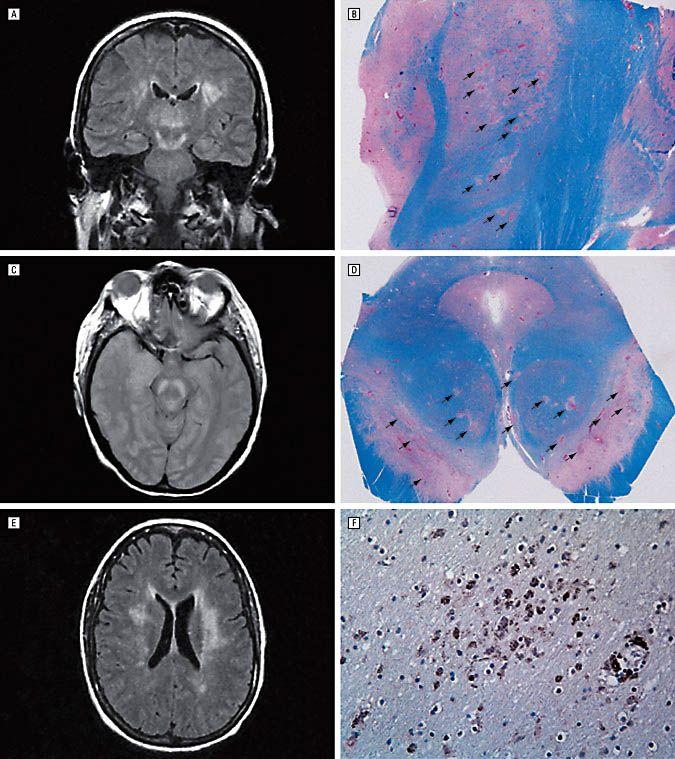
- The following figure demonstrates the correlation between MRI findings and neuropathological changes in a transplant recipient with WNV encephalitis, showing T2/FLAIR hyperintensities in the thalami and deep gray matter structures corresponding to areas of tissue necrosis at autopsy.
- View full figure Figure 1. Naturally Acquired West Nile Virus Encephalomyelitis in Transplant Recipients: Clinical, Laboratory, Diagnostic, and Neuropathological Features. Arch Neurol. July 31, 2004.
13. Special Tests
- EEG: Generalized slowing, triphasic sharp waves — nonspecific but supports encephalopathic process; useful for detecting subclinical seizures[1]
- EMG/nerve conduction studies: Essential to differentiate acute flaccid myelitis (motor axonopathy, preserved sensory potentials) from GBS (demyelinating sensorimotor neuropathy)[1]
- Bedside pulmonary function testing: Negative inspiratory force (NIF) and forced vital capacity (FVC) monitoring in patients with acute flaccid myelitis to detect impending respiratory failure[1]
- Ophthalmologic exam: Slit-lamp and dilated fundoscopy if visual symptoms present[1]
- Cardiac workup (if indicated): Troponin, BNP, echocardiography, cardiac MRI for suspected myocarditis[6]
14. ECG
- Indications: Obtain ECG in all patients with WNV neuroinvasive disease, particularly those with chest pain, dyspnea, hemodynamic instability, or known cardiac risk factors
- WNV-associated cardiac dysrhythmias have been described, including in critically ill ICU patients[2][6]
- If myocarditis suspected: ECG may show sinus tachycardia, nonspecific ST/T-wave changes, ST elevation, conduction delays (AV block, bundle branch block), or ventricular arrhythmias[16-17]
- In a case series of critically ill WNND patients, 4/12 ICU patients had cardiac involvement including suspected myocarditis and Takotsubo syndrome[6]
15. Assessment
- Clinical spectrum: Ranges from mild confusional state to severe encephalopathy, coma, and death[3]
Severity stratification
- Pooled mortality: 9.2% overall; 42.1% require ICU admission[4]
- Mortality 20% in age ≥70; 30–40% in hematologic malignancies/transplant recipients[1]
- Characteristic features distinguishing WNV encephalitis: Extrapyramidal signs (tremor, myoclonus, parkinsonism), acute flaccid paralysis, summer/fall seasonality[1][3]
- Complications: Respiratory failure (from acute flaccid myelitis), seizures, elevated ICP, myocarditis, SIADH/hyponatremia, rhabdomyolysis, secondary infections[1-2][14]
- Long-term sequelae are common: >50% have persistent symptoms — fatigue (37–75%), memory loss (11–57%), concentration deficits (17–48%), depression (17–38%), muscle weakness (7–73%)[1][4]
16. Treatment Plan
Initial stabilization
- ABCs — assess airway protective reflexes; early intubation if bulbar dysfunction or declining respiratory function[1]
- Empiric IV acyclovir (10 mg/kg q8h) until HSV encephalitis is excluded[8]
- Seizure management with benzodiazepines acutely; levetiracetam or other AEDs for recurrent seizures
- IVF resuscitation for dehydration from GI losses or poor oral intake
Supportive care (mainstay of treatment)
- ICU monitoring for encephalitis patients — neuro checks, ICP monitoring if indicated, ventilatory support[1]
- Serial bedside NIF/FVC if acute flaccid myelitis present[1]
- DVT prophylaxis, stress ulcer prophylaxis, glycemic control
- Physical/occupational therapy early in course
Investigational/adjunctive therapies
- IVIG, high-titer WNV IVIG, IFN-α, ribavirin — no proven efficacy; generally not recommended outside of clinical trials[1][9]
- Avoid corticosteroids — associated with increased mortality (aHR 3.93) in a retrospective study[7]
- In transplant recipients: reduce immunosuppression in consultation with transplant team[10]
17. Disposition
- ICU admission: All patients with encephalitis (for airway monitoring, seizure management, ICP concerns), acute flaccid myelitis (respiratory failure risk), or hemodynamic instability[1][4]
- Inpatient (floor): WNV meningitis without encephalopathic features, stable vital signs, able to maintain hydration
- Discharge criteria: Resolving mental status, stable neurologic exam, adequate oral intake, no respiratory compromise, safe home environment
Specialist consultation triggers
- Neurology (all neuroinvasive cases)
- Infectious disease
- Pulmonology/critical care (respiratory failure)
- Ophthalmology (visual symptoms)
- Cardiology (suspected myocarditis)[6]
- PM&R/rehabilitation medicine (early involvement for motor deficits)
- 30–40% of hospitalized patients are discharged to long-term care or rehabilitation facilities[1]
18. Follow Up / Return Precautions
- Follow-up timing: Neurology follow-up within 2–4 weeks of discharge; earlier if new or worsening symptoms
- Expected recovery: Illness duration weeks to months; most motor improvement occurs within the first 4 months after acute flaccid myelitis; cognitive and functional recovery may be prolonged[1]
Return precautions — seek immediate care for
- New or worsening weakness, especially limb weakness or difficulty breathing
- Worsening confusion or decreased alertness
- New seizures
- Difficulty swallowing or speaking
- Chest pain or palpitations
- Long-term monitoring: Screen for depression, cognitive impairment, persistent fatigue at follow-up visits; 9–29% have difficulties with ADLs at 1–18 months[1]
- Patient counseling: No person-to-person transmission; mosquito bite prevention education (EPA-registered repellents, protective clothing, limiting dusk-to-dawn outdoor exposure); no human vaccine available[1]
- Reporting: WNV neuroinvasive disease is a nationally notifiable condition — report to local/state health department[2]
References
1. West Nile Virus. — Gould CV, Staples JE, Guagliardo SAJ, et al. The Journal of the American Medical Association. 2025.
2. West Nile Virus Surveillance and Control Guidelines. — United States Centers for Disease Control and Prevention (2025). 2025.
3. West Nile Virus: Review of the Literature. — Petersen LR, Brault AC, Nasci RS. The Journal of the American Medical Association. 2013.
4. Clinical, Prognostic, and Longitudinal Functional and Neuropsychological Features of West Nile Virus Neuroinvasive Disease in the United States: A Systematic Review and Meta-Analysis. — Roberts JA, Kim CY, Hwang SA, et al. Annals of Neurology. 2025.
5. Neuroinvasive West Nile Virus Infection in Immunosuppressed and Immunocompetent Adults. — Mbonde AA, Gritsch D, Harahsheh EY, et al. JAMA Network Open. 2024.
6. West Nile Virus Neuroinvasive Disease and Cardiac Involvement in Critically Ill Patients in Central Italy: A Case Series. — Tetaj N, Bocci MG, Capecchi G, et al. Frontiers in Medicine. 2026.
7. The Impact of Corticosteroid Therapy on Patients With West Nile Virus: A Retrospective Cohort Study. — Poran I, Basharim B, Leibovici-Weissman Y, et al. The Journal of Infectious Diseases. 2026.
8. State of the Art: Acute Encephalitis. — Bloch KC, Glaser C, Gaston D, Venkatesan A. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2023.
9. Acute Encephalitis in Immunocompetent Adults. — Venkatesan A, Michael BD, Probasco JC, Geocadin RG, Solomon T. Lancet. 2019.
10. Neuroinvasive West Nile virus infection in solid organ transplant recipients. — Kasule SN, Gupta S, Patron RL, Grill MF, Vikram HR. Transplant Infectious Disease : An Official Journal of the Transplantation Society. 2023.
11. West Nile Virus: Epidemiology, Prevention, Clinical Features, Diagnosis, Treatment, and Open Research Questions. — Zerbato V, Rossi B, Di Bella S, et al. Annals of Medicine. 2026.
12. Pearls & Oy-Sters: Bilateral Thalamic Involvement in West Nile Virus Encephalitis. — Guth JC, Futterer SA, Hijaz TA, et al. Neurology. 2014.
13. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
14. Encephalitis. — Binks SNM, Saylor D, Easton A, Thakur KT, Irani SR. Lancet. 2026.
15. Naturally Acquired West Nile Virus Encephalomyelitis in Transplant Recipients: Clinical, Laboratory, Diagnostic, and Neuropathological Features. — Kleinschmidt-DeMasters BK, Marder BA, Levi ME, et al. Archives of Neurology. 2004.
16. 2024 ACC Expert Consensus Decision Pathway on Strategies and Criteria for the Diagnosis and Management Of Myocarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. — Drazner MH, Bozkurt B, Cooper LT, et al. Journal of the American College of Cardiology. 2025.
17. Update on Myocarditis. — Kindermann I, Barth C, Mahfoud F, et al. Journal of the American College of Cardiology. 2012.