Zika Virus Infection
Zika virus (ZIKV) is a mosquito-borne flavivirus transmitted primarily by Aedes species mosquitoes, with 50–80% of infections being asymptomatic and symptomatic cases typically presenting as a mild…
Zika virus (ZIKV) is a mosquito-borne flavivirus transmitted primarily by Aedes species mosquitoes, with 50–80% of infections being asymptomatic and symptomatic cases typically presenting as a mild, self-limited illness lasting up to one week.[1-2] The critical clinical significance lies in its association with congenital Zika syndrome (microcephaly and brain anomalies) and Guillain-Barré syndrome (GBS).[1][3]
1. History
- Travel history is paramount: recent travel to or residence in areas with active or past ZIKV transmission (tropics/subtropics, particularly the Americas, Southeast Asia, Pacific Islands)[2][4]
- Incubation period: 3–14 days[1]
- Symptom characterization: acute onset of maculopapular rash (often pruritic), low-grade fever, arthralgia/myalgia, and non-purulent conjunctivitis[1-2][5]
- Other symptoms: headache, retro-orbital pain, edema, lymphadenopathy, vomiting[2]
- Duration: typically up to 7 days, self-limited[1][6]
- Sexual exposure: unprotected sex with a partner who traveled to an endemic area, even if asymptomatic[2][4]
- Pregnancy status: essential to determine immediately — both symptomatic and asymptomatic infections pose risk for vertical transmission[1][4]
- Prior flavivirus exposure: history of dengue, yellow fever, or yellow fever vaccination (complicates serologic interpretation)[1]
2. Alarm Features
- Rapidly progressive ascending weakness → suspect GBS (onset typically 5–10 days after acute illness)[1][7]
- Bilateral facial paralysis — seen in 50% of ZIKV-associated GBS cases[7]
- Respiratory insufficiency in the setting of progressive weakness[8]
- Pregnancy with confirmed or suspected ZIKV exposure — regardless of symptoms[4][9]
- Severe thrombocytopenia, hemorrhagic manifestations (consider dengue co-infection)[2]
- Encephalopathy, meningoencephalitis, acute myelitis, uveitis — rare but reported[2]
3. Medications
- No specific antiviral therapy exists[1-2]
- Supportive care: acetaminophen for fever and pain[2]
- Avoid aspirin and NSAIDs until dengue is ruled out (hemorrhage risk)[2][10]
- GBS treatment: IVIG or therapeutic plasma exchange, same as classic GBS[1][11]
- No approved vaccine currently available; multiple candidates in clinical trials[1]
4. Diet
- Adequate oral hydration is the primary dietary recommendation during acute illness[2]
- No specific dietary triggers or restrictions
- Encourage rest and fluid intake, particularly in febrile patients or those with vomiting
5. Review of Systems
- Neurologic: weakness, paresthesias, difficulty walking, facial droop, diplopia, dysphagia (GBS screening)[1][7]
- Musculoskeletal: arthralgia, myalgia — distinguish from chikungunya (which causes more severe/prolonged joint symptoms)[2]
- Ophthalmologic: conjunctivitis (non-purulent), visual changes (uveitis)[2]
- Dermatologic: rash character — diffuse maculopapular, often pruritic[5-6]
- OB/GYN: pregnancy status, last menstrual period, plans for conception[4]
- Hematologic: easy bruising, bleeding (to evaluate for dengue)[2]
6. Collateral History and Family History
- Travel companions with similar symptoms (cluster identification)
- Sexual partners' travel history and symptom status[2][4]
- Household members — mosquito exposure risk assessment
- Family history is not a significant contributor to ZIKV susceptibility
- Social context: occupation involving outdoor exposure in endemic areas, housing conditions (screens, air conditioning)[10]
- Report suspected cases to state/local health departments — nationally notifiable condition[2]
7. Risk Factors
- Travel to or residence in endemic areas (Latin America, Caribbean, Southeast Asia, Pacific Islands)[2][4]
- Unprotected sexual contact with an infected or exposed partner[4]
- Living in areas with Aedes aegypti or Aedes albopictus mosquito populations[6]
- Lack of mosquito bite prevention (no repellent, no screens, standing water near residence)[10]
- Pregnancy — not a risk factor for infection but dramatically increases clinical significance[3-4]
- Blood transfusion (rare but documented route)[6]
- Laboratory exposure[4]
8. Differential Diagnosis
Per CDC guidance, the differential includes
- Dengue fever — most important to distinguish; similar geography and presentation but with higher risk of hemorrhage and shock; typically higher fever, more severe myalgia, thrombocytopenia, and leukopenia
- Chikungunya — more prominent and debilitating polyarthralgia, often symmetric
- Malaria — cyclical fevers, rigors, hepatosplenomegaly; thick/thin smear
- Measles — cephalocaudal rash progression, Koplik spots, cough/coryza/conjunctivitis triad
- Rubella — similar rash and lymphadenopathy; critical to distinguish in pregnancy
- Leptospirosis — conjunctival suffusion, jaundice, renal failure
- Parvovirus B19 — "slapped cheek" rash, arthralgias
- Rickettsiosis — eschar, petechial rash
- Oropouche virus — emerging arbovirus with overlapping geography
- Enterovirus, adenovirus, group A streptococcal infection[2]
9. Past Medical History
- Prior flavivirus infections (dengue, yellow fever, West Nile) — affects serologic interpretation and may influence immune response[1-2]
- Yellow fever vaccination history[2]
- Prior GBS episodes (increased vigilance for recurrence)
- Pregnancy history, prior adverse pregnancy outcomes
- Immunocompromised states — limited data on impact but relevant for clinical monitoring
- Autoimmune conditions (relevant if GBS develops)
10. Physical Exam
- Vital signs: low-grade fever (often <38.5°C); typically hemodynamically stable[1]
- Skin: diffuse maculopapular rash, often pruritic; may be confluent[5-6]
- Eyes: bilateral non-purulent conjunctivitis; fundoscopic exam if visual complaints (uveitis)[2]
- Lymph nodes: lymphadenopathy may be present[2]
- Joints: tenderness without significant swelling (distinguish from chikungunya)
Neurologic exam (critical)
- Cranial nerves — facial nerve palsy[7]
- Motor strength — proximal and distal, ascending pattern
- Deep tendon reflexes — areflexia suggests GBS[8]
- Sensory exam
- Gait assessment
- Abdominal exam: hepatosplenomegaly absent (if present, consider dengue or malaria)
11. Lab Studies
- NAAT (RT-PCR) on paired serum and urine — preferred diagnostic test; perform within first 1–2 weeks of illness[1-2]
- For symptomatic pregnant women: NAAT on serum and urine ASAP, up to 12 weeks after symptom onset[9]
- Positive NAAT on a single sample should be re-extracted and re-tested to rule out false positive[9]
- IgM serology: develops end of first week; persists months to years; cross-reacts with dengue — no longer recommended for pregnant women per updated IDSA/CDC guidance[1][9]
- PRNT (plaque reduction neutralization test): confirmatory but limited to reference labs; still subject to cross-reactivity in secondary flavivirus infections[1-2]
- Concurrent dengue testing is recommended (NAAT and IgM) given overlapping geography and presentation[9][12]
- CBC: may show mild leukopenia, thrombocytopenia[2]
- Per current CDC guidance, non-pregnant patients should not be routinely tested for Zika given very limited current transmission; assess for dengue instead[9]
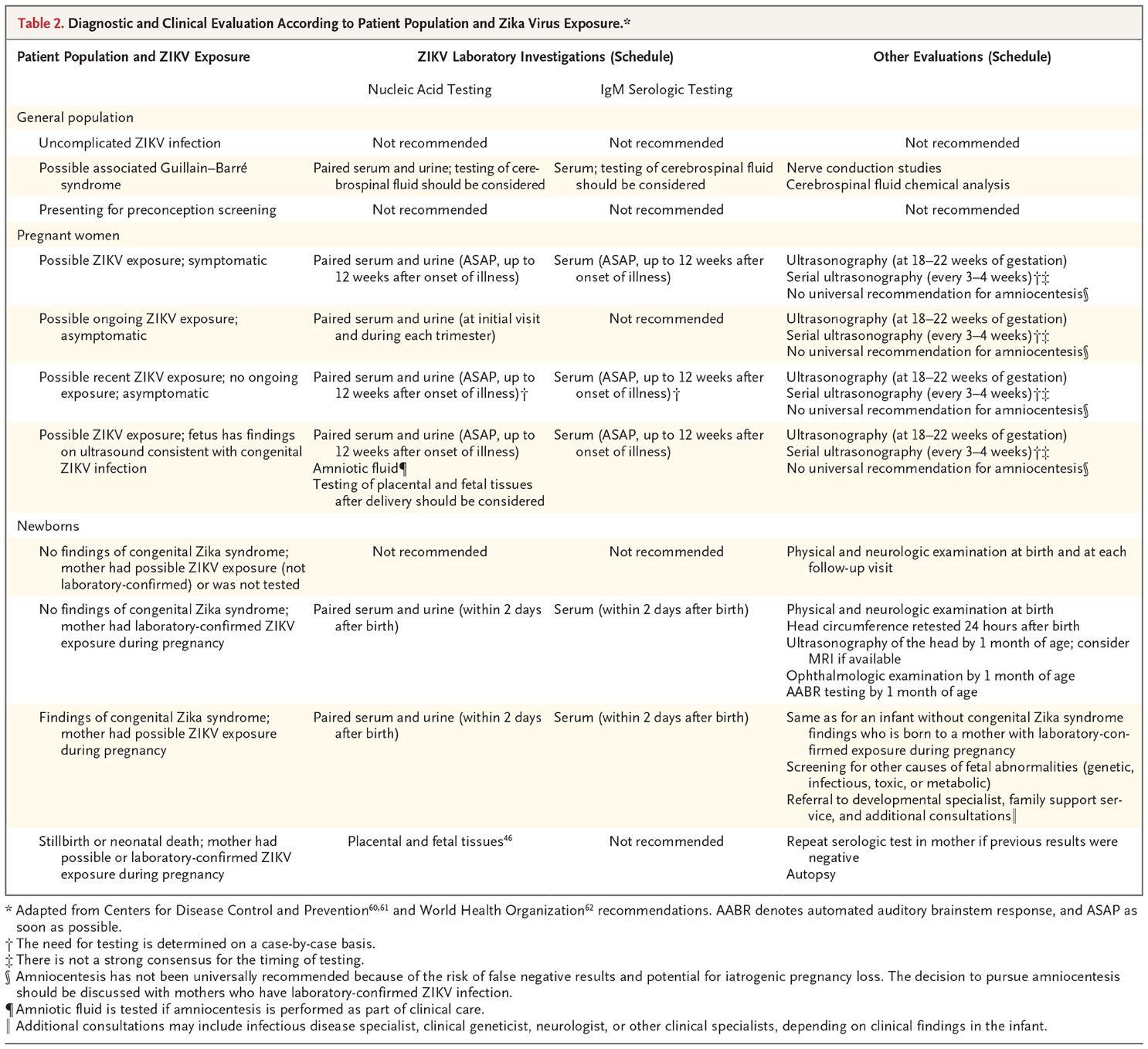
- The following table from the NEJM summarizes the diagnostic and clinical evaluation approach stratified by patient population:
- View full figure Table 2. Diagnostic and Clinical Evaluation According to Patient Population and Zika Virus Exposure.* Zika Virus Infection — After the Pandemic. N Engl J Med. October 9, 2019.
12. Imaging
- Not routinely indicated for uncomplicated ZIKV infection in adults
Pregnant women with confirmed/suspected ZIKV
- Fetal ultrasound at 18–22 weeks gestation[1]
- Serial ultrasound every 3–4 weeks to monitor for microcephaly, ventriculomegaly, intracranial calcifications[1][13]
- Amniocentesis is not routinely recommended (risk of false negatives, iatrogenic loss)[1]
- Newborns with congenital Zika syndrome: head ultrasound by 1 month; consider MRI if available[1]
- GBS: MRI of spine may show nerve root enhancement; primarily a clinical/electrodiagnostic diagnosis
13. Special Tests
- Nerve conduction studies/EMG: indicated if GBS suspected; ZIKV-associated GBS shows AIDP (most common) or AMAN subtypes[7][11]
- CSF analysis: in GBS — albuminocytologic dissociation (elevated protein, normal cell count); ZIKV NAAT on CSF should be considered[1]
- Tourniquet test: if dengue is being considered
- Ophthalmologic examination: for infants with congenital Zika syndrome (posterior and anterior segment anomalies); for adults with visual complaints[13]
- AABR (automated auditory brainstem response): for newborns with suspected congenital ZIKV infection, by 1 month of age[1]
14. ECG
- Not routinely indicated for uncomplicated ZIKV infection
- Consider ECG if myocarditis is suspected (rare) or in critically ill patients with GBS requiring ICU-level care (autonomic dysfunction monitoring)
- GBS-associated cardiac arrhythmias from autonomic instability warrant continuous telemetry
15. Assessment
- Typical presentation: mild, self-limited febrile illness with rash, arthralgia, and conjunctivitis in a returning traveler from an endemic area; resolves within 1 week[1-2]
- Atypical/severe presentations: GBS (2–3 per 10,000 infections), encephalopathy, myelitis, severe thrombocytopenia — rare but potentially fatal[1-2]
Severity stratification
- Mild: uncomplicated febrile illness → outpatient management
- Moderate: significant dehydration, inability to tolerate PO → observation
- Severe: neurologic complications (GBS with respiratory compromise), pregnancy with fetal anomalies → admission
- Congenital Zika syndrome: microcephaly, parenchymal/cerebellar calcifications, ventriculomegaly, arthrogryposis, ocular anomalies, low birth weight[13]
16. Treatment Plan
Acute uncomplicated infection
- Acetaminophen for fever and pain[2]
- Oral hydration and rest[2]
- Avoid aspirin/NSAIDs until dengue excluded[2][10]
- Mosquito bite prevention during first week of illness to prevent onward transmission[2]
Pregnancy
- Urgent NAAT testing on serum and urine[9]
- Concurrent dengue NAAT and IgM[12]
- Serial fetal ultrasound monitoring[1]
- OB/MFM referral for co-management[2]
GBS
- IVIG (0.4 g/kg/day × 5 days) or therapeutic plasma exchange[1][11]
- ICU admission if respiratory compromise or rapid progression
- Respiratory monitoring (FVC serially)
- DVT prophylaxis, physical therapy
Prevention counseling
- Mosquito bite avoidance: DEET-containing repellents, permethrin-treated clothing, screens, air conditioning[10]
- Sexual transmission prevention: condoms for 3 months (male partner) or 2 months (female partner) after suspected infection[1]
- Pregnant women should avoid travel to endemic areas[4]
17. Disposition
- Discharge (majority): uncomplicated illness with adequate PO intake, no neurologic symptoms, non-pregnant or with OB follow-up arranged[1][4]
- Observation: dehydration requiring IV fluids, pregnant patients awaiting urgent testing
Admission criteria
- Progressive neurologic deficits (GBS)[11]
- Respiratory compromise
- Severe thrombocytopenia or hemorrhagic manifestations
- Encephalopathy or meningoencephalitis[2]
Specialist consultation triggers
- Neurology: any suspected GBS or CNS complication
- MFM/OB: any pregnant patient with confirmed or suspected exposure
- Infectious disease: diagnostic uncertainty, complex serologic interpretation
- Pediatric neurology/developmental specialist: congenital Zika syndrome[1]
18. Follow Up / Return Precautions
- Follow-up timing: PCP or infectious disease within 1–2 weeks for symptom resolution; pregnant patients per OB schedule with serial ultrasounds[1]
Return immediately for
- Weakness in arms or legs, difficulty walking or breathing (GBS)[1]
- Facial droop or difficulty swallowing
- Severe headache, altered mental status, seizures
- Signs of hemorrhage (if dengue not yet excluded)
Patient counseling
- Expected recovery: symptoms resolve within 5–7 days[1]
- Use mosquito protection for at least 1 week after illness onset to prevent transmission[2]
- Use condoms or abstain from sex per recommended timeframes to prevent sexual transmission[1]
- If planning pregnancy, defer conception per CDC guidance[4]
- Nationally notifiable disease — ensure reporting to state/local health department[2]
References
1. Zika Virus Infection — After the Pandemic. — Musso D, Ko AI, Baud D. The New England Journal of Medicine. 2019.
2. Zika. — Stacey W. Martin, Dana Meaney-Delman, and J. Erin Staples CDC Yellow Book. 2025.
3. Zika Virus Infection as a Cause of Congenital Brain Abnormalities and Guillain-Barré Syndrome: Systematic Review. — Krauer F, Riesen M, Reveiz L, et al. PLoS Medicine. 2017.
4. Zika Virus: Common Questions and Answers. — Igbinosa II, Rabe IB, Oduyebo T, Rasmussen SA. American Family Physician. 2017.
5. Travel-Associated Zika Virus Disease Cases Among U.S. Residents--United States, January 2015-February 2016. — Armstrong P, Hennessey M, Adams M, et al. MMWR. Morbidity and Mortality Weekly Report. 2016.
6. Zika Virus: Report From the Task Force on Tropical Diseases by the World Federation of Societies of Intensive and Critical Care Medicine. — Silva GS, Richards GA, Baker T, et al. Journal of Critical Care. 2018.
7. Guillain–Barré Syndrome Associated with Zika Virus Infection in Colombia. — Parra B, Lizarazo J, Jiménez-Arango JA, et al. The New England Journal of Medicine. 2016.
8. Guillain-Barré Syndrome. — Shahrizaila N, Lehmann HC, Kuwabara S. Lancet. 2021.
9. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
10. Zika Virus—What the Otolaryngologist Should Know: A Review. — Arnaoutakis D, Padhya T. JAMA Otolaryngology-- Head & Neck Surgery. 2017.
11. An Update on Zika Virus Infection. — Baud D, Gubler DJ, Schaub B, Lanteri MC, Musso D. Lancet. 2017.
12. Dengue and Zika Virus Diagnostic Testing for Patients With a Clinically Compatible Illness and Risk for Infection With Both Viruses. — Sharp TM, Fischer M, Muñoz-Jordán JL, et al. MMWR. Recommendations and Reports : Morbidity and Mortality Weekly Report. Recommendations and Reports. 2019.
13. Congenital Zika Syndrome: A Systematic Review. — Freitas DA, Souza-Santos R, Carvalho LMA, et al. PloS One. 2020.